The place of modern enterosorption in the treatment of children with allergic dermatoses
THE PLACE OF MODERN ENTEROSORPTION IN THE TREATMENT OF CHILDREN WITH ALLERGIC DERMATOSES
E.N. Okhotnikova, K.V. Mellyna, L.V. Bondarenko, I.V. papa
National medical academy of postgraduate education named after P.L. Shupyka, Kyiv
Consultative and diagnostic polyclinic of the National Children's Specialized Hospital "OHMATDET"
Resume. The experience of using the drug "Atoxyl" in the complex therapy of allergic diseases (hives, atopic dermatitis) in children is shown. Enterosorbent Atoxyl has proven itself as an effective and important component of the complex therapy of alimentary-dependent allergic pathology. The use of Atoxyl allows to reduce the duration of the acute period of AD, urticaria and Quincke's edema in children and to reduce the course dose of systemic corticosteroids.
Key words: allergic diseases, complex therapy, enterosorbents, Atoxyl.
Introduction
Allergic diseases in children are widespread and lead among diseases of other etiologies. According to experts' forecasts, the 21st century will be characterized by the further growth of this pathology. Allergic dermatoses occupy a leading place in this group of diseases and are represented by a large number of nosological forms, including atopic dermatitis (AD), urticaria (K), Quincke's edema, medicinal allergic vasculitis, etc.
Allergy is currently considered a systemic pathology, and even in those cases where one organ is affected, there is always a risk of systemic manifestations. The formation of allergy in children is characterized by the stages of development of sensitization and the transformation of clinical manifestations of atopy depending on the age of the child. Most clinicians note the "rejuvenation" of allergic diseases, an increase in the specific weight of severe drug-resistant forms, and a tendency toward a chronic course.
Often in children with atopy, its manifestation manifests itself already in early childhood in the form of food allergy and AD, later allergic rhinitis and bronchial asthma are added. According to modern concepts, the severe course of AD and allergic rhinitis are risk factors for the subsequent development of bronchial asthma and other systemic manifestations of allergy.
The results of numerous studies indicate that allergic skin diseases, as a rule, occur against the background of concomitant pathology of the gastrointestinal tract and hepatobiliary system, the syndrome of excessive bacterial growth.
The digestive system, in direct contact with a huge number of foreign proteins, along with the nutritional function, provides protection of the body's internal environment from the influence of antigens of various origins: food, microbial, viral, fungal, and parasitic.
In physiological conditions, there are a number of barriers in the digestive system, represented by anatomical, physiological and immune factors, which prevent the penetration of food antigens into the internal environment of the body, where they induce an immune response. The failure of the above-mentioned barriers is more often manifested in childhood, which is connected with the anatomical and physiological features of the gastrointestinal tract. Damage to the barriers of the digestive tract as a result of inflammatory, infectious and parasitic diseases promotes food sensitization.
Recently, a lot of attention has been paid to disorders of not only cavity, but also parietal digestion. Inadequate digestion of proteins has a toxic effect and contributes to an increase in the permeability of the mucous membranes of the digestive tract. The liver is one of the main effector organs of the phagocytic mononuclear system. It is involved in the capture and elimination, first of all, of antigens of intestinal origin. Food allergies can occur when large protein molecules or their fragments pass through the liver filter, retaining their antigenic properties. In addition, the increased permeability of the small intestine allows a large amount of histamine to be absorbed with its subsequent entry into the bloodstream, since the possibilities of histamine to inactivate it are limited. A decrease in the functional activity of the pancreas, a decrease in the acidity of gastric juice, and dysbiotic processes in the intestine also contribute to the massive influx of antigens from the intestine into the blood circulation.
The development of allergic reactions in the syndrome of excessive bacterial growth is associated with the increased reproduction of histamineogenic flora, which increases the amount of histamine in the body by decarboxylation of food histidine. It is also important to reduce the production of histamine by the damaged intestinal lining. Products of the metabolism of microorganisms can also be allergens.
The development of pathological reactions to food can be carried out by various mechanisms. The true food allergy is based on an immunological IgE-mediated reaction. The pathological process, which is similar to allergy in terms of clinical manifestations, but does not have an immunological phase of development, when the pathochemical and pathophysiological stages coincide, is characterized as pseudoallergy. A. Andersen (1984) distinguishes 5 types of non-immune reactions in the formation of food allergy symptoms:
- anaphylactoid reactions due to food histamine liberators;
- reactions to food additives;
- reactions to pharmacological agents coming from food;
- reactions caused by enzymopathies;
- reactions to food toxins (bacterial or food origin).
There are 3 generally recognized groups of mechanisms that play a leading role in the pathogenesis of food pseudoallergy:
- histamine;
- violation of complement system activation;
- violation of arachidonic acid metabolism.
Despite the various ways of the formation of pathological reactions to food, all of them are accompanied by the development of an endogenous intoxication syndrome of varying degrees of severity, the clinical manifestations of which are general weakness, irritability, sleep and appetite disturbances, decreased concentration, changes in the body's temperature response, muscle pain, etc. Often, the intoxication syndrome is weakly expressed or is in a latent stage.
Endotoxinemia syndrome is associated with the accumulation of products of physiological metabolism in excess concentrations: pyruvate, lactate, creatinine, bilirubin, urea, products of impaired metabolism (ketones, aldehydes, alcohols, ammonia, carboxylic acids), mediators of inflammation, biogenic amines, cytokines, prostaglandins, microbial toxins, various antigens and immune complexes.
To normalize homeostasis in the complex treatment of patients with allergic dermatoses, modern detoxification methods are widely used. The most simple, convenient and effective method is enterosorption, which has found wide application in the treatment of allergic diseases, both in the acute period of the process and during remission.
The use of modern enterosorbents has a direct effect on the sorption from the intestinal lumen of allergens, xenobiotics, exotoxins, mediators of anaphylaxis, biologically active substances, prevents the formation of circulating immune complexes, which indirectly reduces the burden on the immune system, detoxification organs, normalizes the imbalance of biologically active substances and microbiocenosis in the human body.
Sorbents that are recommended for use in pediatrics, in the form of oral forms, must meet the following requirements:
- have a high selective sorption capacity;
- be relatively inert in the intestinal lumen;
- minimally absorb useful substances;
- will not cause trauma or any reactive changes in intestinal tissues;
- not be toxic;
- evacuate well from the intestines;
- not have an unpleasant taste and smell;
- be convenient for use in children.
Silicon dioxide, which is a microspherical ultra-high-dispersion enterosorbent of the new 4th generation (the area of active sorption is greater than 400 m2 for 1 g of substance), has pronounced sorption properties that meet these requirements. It has pronounced sorption, detoxification and antimicrobial properties. The drug is produced under the trade name "Atoxyl". It promotes absorption from the gastrointestinal tract and the removal from the body of exo- and endogenous toxic substances of various origins (including products of the life cycle of pathogenic microorganisms, food and bacterial allergens).
Materials and research methods
On the basis of the Consultative Diagnostic Polyclinic of the National Children's Specialized Hospital "OKHMATDET", a study was conducted to study the effectiveness and tolerability of "Atoxyl" as part of complex therapy in children with AD and relapsing urticaria.
The work was conducted as an open randomized study by the method of random selection of patients.
Research design:
The main groups are children who received treatment with the drug "Atoxyl":
- 1st group — 30 children aged from 1 to 5 years old, suffering from AD;
- 2nd group — 18 children aged 2 to 15 years, with acute (10 children) (OK) and recurrent (8 children) urticaria (RK);
The comparison groups consisted of children whose age, nosological form, and severity of the disease were comparable to children of the main groups, but whose treatment complex did not include an enterosorbent:
- 1st group — 10 children with AD;
- 2nd group — 10 children with urticaria.
Indications for the appointment of Atoxyl were the acute phase of the allergic process. The duration of use of Atoxyl was 5–10 days at a daily dose of 150 mg/kg. The drug was prescribed orally in the form of a dry substance diluted in water, 1–1.5 hours before meals and 2 times a day between doses. In patients with acute inflammatory manifestations of AD, characterized by wetting, Atoxyl was also used externally in the form of a powder.
Diagnostic support included: allergy anamnesis data, analysis of "food diary" data, clinical manifestations and their dynamics, ultrasound results of abdominal organs, level of total IgE and specific IgE-antibodies to various, including food, allergens determined by the ELISA method in the dynamics of observation, stool analysis for the amount and composition of microbial flora, coprogram, stool culture for flora, three-fold measurement of indicators - before treatment (0 day), on 7th and 14th days of the study, as well as similar systemic and external therapy (for AD).
The effectiveness of treatment was evaluated based on the dynamics of the following criteria: the SCORAD index (AD), the level of general and allergen-specific IgE, signs of damage to the gastrointestinal tract, the degree of dysbacteriosis (AD), the level of hematological activity (AC), the total dose of systemic corticosteroids (with AC), the duration of the acute period of each process.
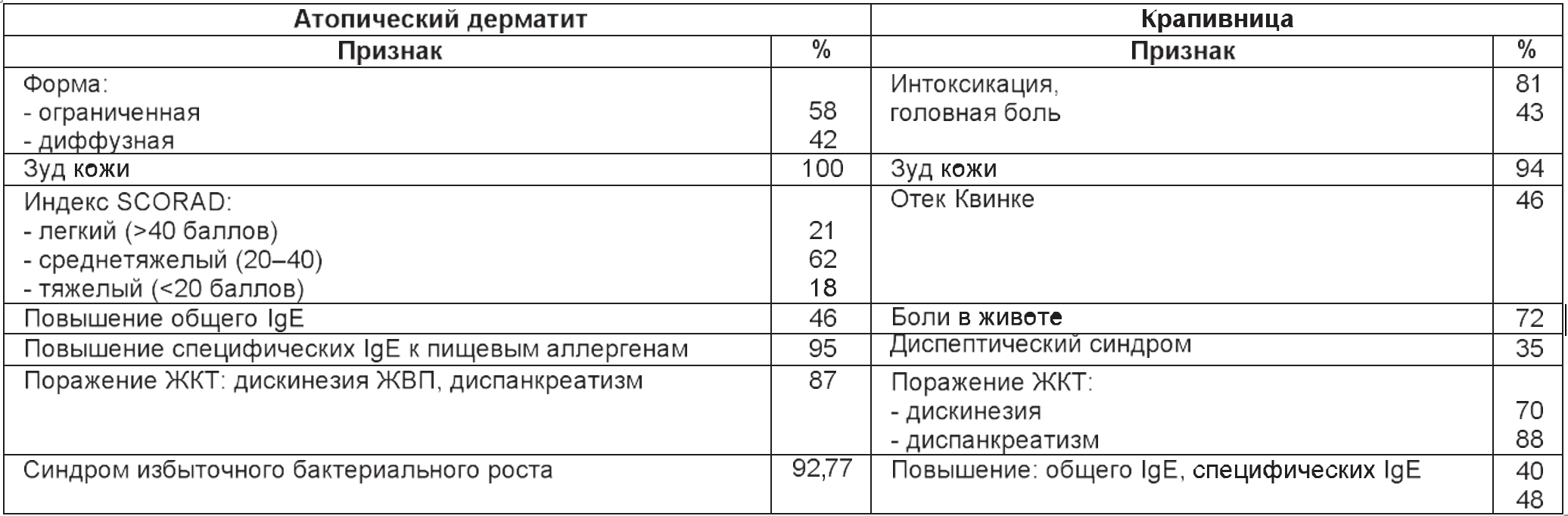
The clinical characteristics of the examined children are presented in the table.
Table
Characteristic contingents children (%)
Research results and their discussion
The analysis of the obtained data showed that in the children of the main groups, on the background of the use of the drug "Atoxyl", favorable dynamics of clinical manifestations were noted in the form of a decrease in the severity of objective symptoms (edema, hyperemia, rash, crusts), a decrease in the intensity of itching and disturbed sleep, which was manifested in a significant decrease in the integrative index SCORAD (Fig. 1).
The assessment of the dynamics of AD flow showed that, against the background of the use of enterosorbent, the signs of severe flow leveled out: the number of children with moderate flow decreased by 6.81 TP3T, and the number of children with mild flow of AD increased by 24.41 TP3T. The most resistant to therapy were children with sensitization to aeroallergens and food allergens, as well as patients with a diffuse form of AD.
Against the background of the therapy, hyperemia, edema and inflammatory infiltration of the skin on the face regressed more actively than in other areas. In children of early age, clinical improvement began earlier, and skin manifestations were easier to treat than in children 3–5 years old, in whom areas of the skin in the area of the elbow bends were slowly treated.
The area of rash and the intensity of objective symptoms proportionally decreased in all children already after 7 days of treatment. The study of the dynamics of itching showed that already after 1 week its severity decreased significantly (by 2.0–2.5 times). By the end of the 2nd week, weak manifestations of itching were noted only in 7 patients (24%). The children became calmer, sleep was restored.
After 7 days, there was a decrease in the level of specific IgE to food allergens by 25–30% in children receiving complex therapy, and after 14 days — by 35–40%. In 3 patients of the 1st group with pronounced manifestations of eczema with wetting after external application of Atoxyl, a significant reduction in itching and soreness of the skin in the area of the lesion was noted.
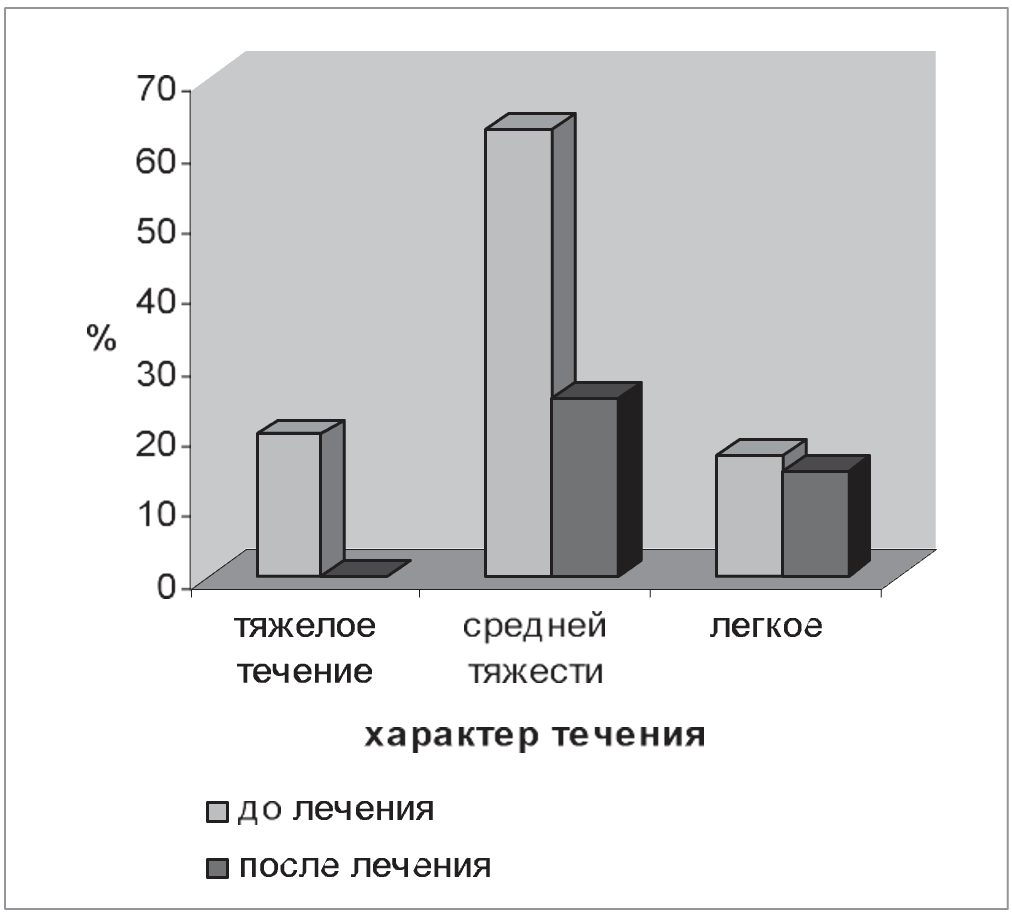
Rice. 1. Dynamics of AD flow (SCORAD index) against the background of Atoxyl application
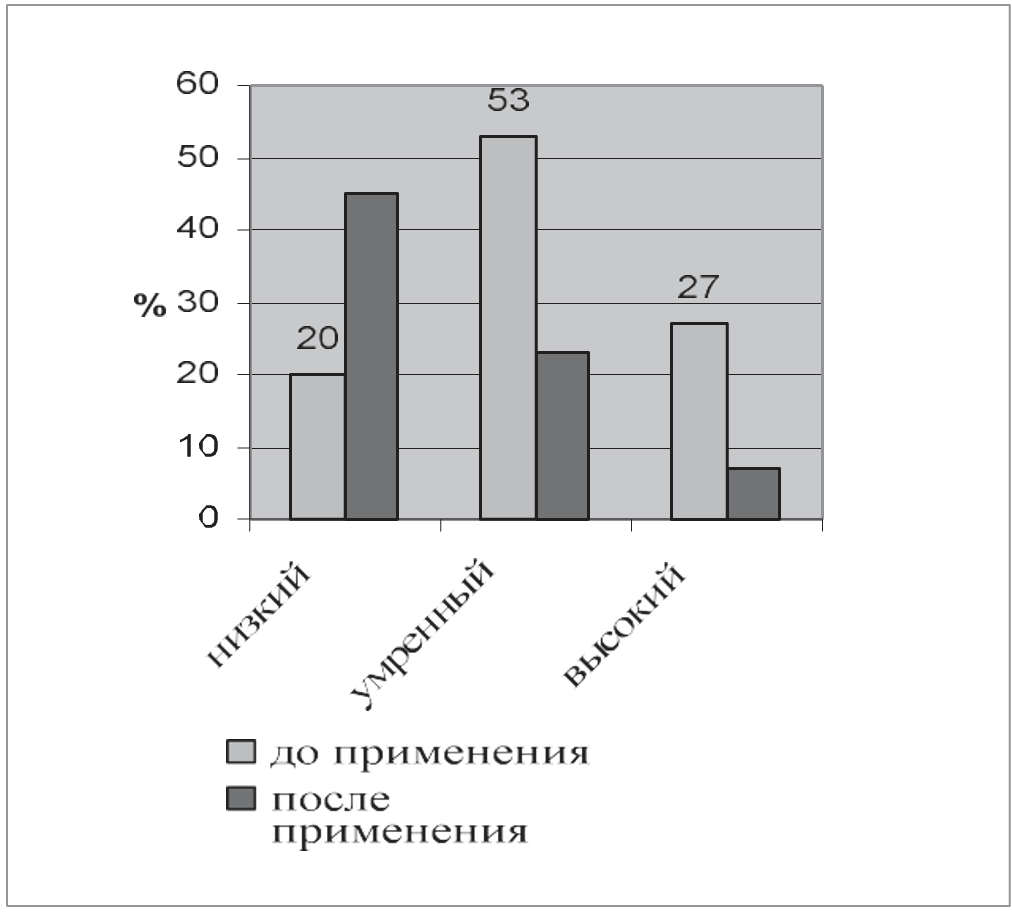
Fig. 2. Dynamics of the level of specific IgE to cow's milk proteins in children with AD after the use of Atoxyl
Figure 2 shows the dynamics of the level of specific IgE to cow's milk proteins.
Against the background of treatment with an enterosorbent in children with allergic skin diseases, intestinal microbiocenosis disorders manifested by a deficiency of bifidobacteria and lactobacilli, an increase in the number and a change in the species ratio of opportunistic bacteria normalized. In the dynamics, there was a significant increase to the normal level of the population of bifidobacteria and lactobacilli in children who used Atoxyl and had an initial reduced level of these bacteria. Along with this, a clear positive trend in representatives of the conditionally pathogenic microflora of feces was revealed. Upon re-examination of feces against the background of Atoxyl application, normalization of intestinal microbiocenosis was noted in 14 (78%) children, and without the appointment of probiotics. In the children of the comparison group, normalization of the intestinal flora was either not observed, or occurred later (Fig. 3).
The use of Atoxyl in children of the main group with acute and exacerbation of recurrent urticaria contributed to the improvement of the patients' condition: on the 2nd day of application - in 48.8% children, on the 3rd day - in 41.4%, which was manifested by a decrease in each itch and the absence of new rashes. The symptoms of flatulence stopped, the stool normalized. According to the survey of children and their parents, on the 2nd day of use, an improvement in the general condition of almost all patients (96%) was noted: anxiety and irritability decreased due to a decrease in the intensity of itching, and appetite improved. In 13% children, the symptoms of acute urticaria stopped within 1 day, one child had a recurrent course.
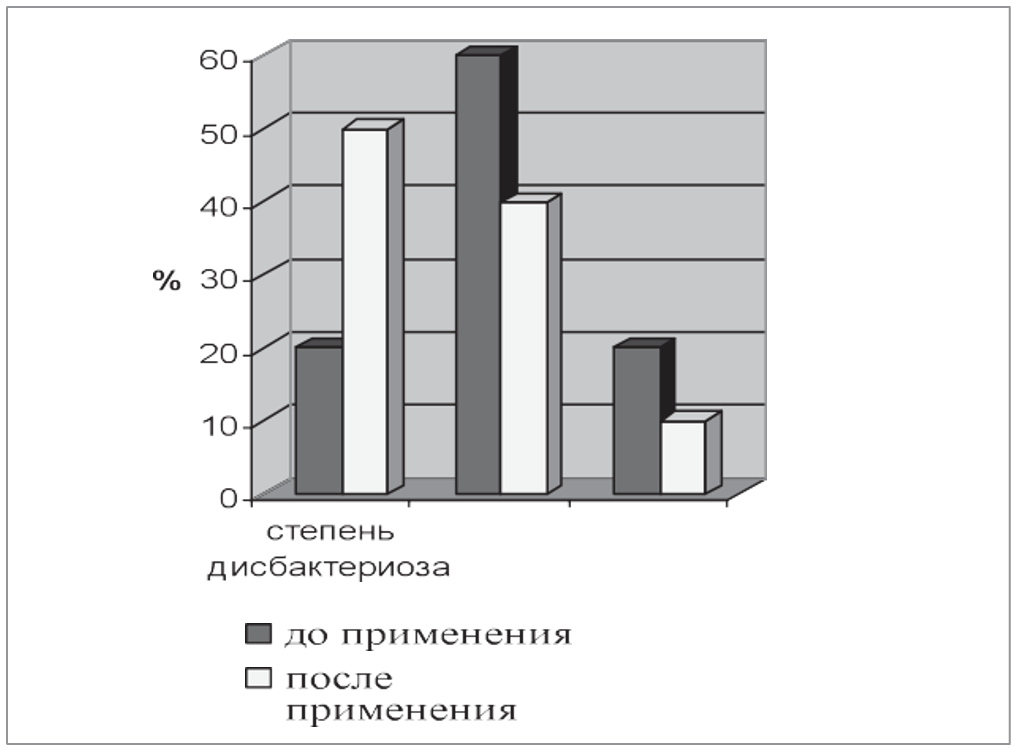
Rice. 3. Dynamics of the degree of dysbacteriosis in children with AD against the background of the use of Atoxyl

Fig. 4. Dynamics of symptoms of urticaria against the background of the use of Atoxyl
In the children of the comparison group, who did not receive Atoxyl, positive dynamics were noted on the 4th–5th day. Normalization of laboratory indicators of blood activity was noted in 76% children who received enterosorbent on the 5th day, on the 6th — in 22% patients, on the 7th — in 13% children. In the patients of the comparison group, the improvement of these parameters was noted by the 7–8 day of therapy (Fig. 4).
Thus, the use of an enterosorbent accelerated the positive dynamics of clinical manifestations in children with acute urticaria and made it possible to reduce the duration and course dose of systemic glucocorticoids (GCS). The obtained results correlate with literature data that enterosorbents increase the sensitivity of GCS receptors, allowing to reduce the volume of GCS therapy by an average of 2 times.
Clinical improvement after the end of complex therapy with the inclusion of Atoxyl was recorded in 94.61 TP3T children. At the same time, clinical remission was achieved in 65.6% patients, significant improvement in 24.3% children, improvement in 6.6% children, and only 3.5% children had no effect. Children took Atoxyl without any complications.
In no case were there any changes in the basic biochemical constants of the body. Side effects in the form of dyspepsia or allergic reactions were not revealed. It should be noted the good organoleptic properties of the sorbent: children, even young ones, did not refuse to take the drug.
Thus, the enterosorbent Atoxyl has proven itself as an effective and important component of the complex therapy of food-dependent allergic pathology. Its use allows to reduce the duration of the acute period of AD, urticaria and Quincke's edema in children, as well as to reduce the course dose of systemic corticosteroids.
Conclusions
- Atoxyl is a modern enterosorbent with unique properties and good tolerance by children of any age.
- The inclusion of enterosorbent Atoxyl in the complex therapy of AD and urticaria is pathogenetically justified and clinically expedient.
- The effectiveness of Atoxyl has been convincingly proven in patients with a significant food allergy, which was manifested by a reduction in the duration of the acute period of AD, urticaria, and Quincke's edema, a decrease in the level of specific IgE to cow's milk proteins, an improvement in the condition of the gastrointestinal tract (including the degree of bacterial overgrowth syndrome), a decrease in the total dose of systemic corticosteroids in children with an acute episode of urticaria and Quincke's edema.
LITERATURE
- Atopic dermatitis: [handbook for doctors] / under the editorship. Yu. V. Sergeeva. — M.: Medicine for all, — pp. 181-183.
- Atopic dermatitis: [handbook for doctors] / Ed. Prof. T. V. Protsenko. — 2nd ed., revised. — Donetsk: Vostochnyi izdatelskii dom, —128 p.
- Balabolkin I. I. Atopic dermatitis in children / I. I. Balabolkin. — Moscow: Medicine, 1999. — 238 p.
- Belyakov N. A. Enterosorption (introduction to the problem) / N. A. Belyakov A. V. Solomennikov. — L., — 35 p.
- Kalyuzhnaya L. D. Atopic dermatitis. Contemporary questions of diagnosis and treatment / L. D. Kalyuzhnaya // Klin. immunol., allergol. and infectol. — — No. 1. — P. 19-22.
- Kozlov S.V. Influence of various enterosorbents and enteral nutrition on chyme, intoxication, digestive and absorptive function of the intestines / S.V. Kozlov // Abdominal surgery. — Yaroslavl, — pp. 119-121.
- Lysykov Yu. A. Application of sorption technologies in surgical practice / Yu. A. Lysykov // Sat. works on the use of Enterosgel in medicine. — M., 2002. — Part I. — pp. 13-16.
- Nagornaya N. V. Use of enterosorption in the treatment of atopic dermatitis / N. V. Nagornaya, E. V. Bordyugova, A. V. Dubovaya // Sovr. pediatrics.— — No. 4(9). - pp. 67-70.
- Paliy I.G. Use of the enterosorbent Enterosgel in the complex treatment of diseases accompanied by skin allergic manifestations (brief overview of the literature) / I.G. Paliy, I.G. Reznychenko // Medical and biological aspects of the use of the enterosorbent Enterosgel for the treatment of various diseases: sb. science works - K., 2004. - P. 48-51.
- Shchelkunov L.F. Enterosorbents of ecologically harmful substances — an important group of food additives in the human diet / L.F. Shchelkunov // Modern problems of toxicology. — 2003. — No. 4. — P. 68-73.
- Growth pattern of breastfed and non-breastfed infants with atopic dermatitis in the first year of life / Agostoni, Grandi F., Scaglioni S. [et al.] // Pediatrics. — 2000. — Vol. 106 (5).
- Is atopy increasing? / Nakagomi, Itaya H., Tominaga T. [et al.] // Lancet. — 1994. — Vol. 343. — R. 121-122.