Comparative evaluation of the use of the enterosorbent Atoxil
UDC 616.379-008.64:617.586-002.3/.4]-085
COMPARATIVE ASSESSMENT OF THE USE OF ENTEROSORBENT "ATOXYL" IN THE COMPLEX TREATMENT OF PURULOUS-NECRotic PATIENTS WITH DIABETIC FOOT SYNDROME.
S.M. Antonyuk, A.A. Derevyanko, V.B. Akhrameev, P.F. Golovnia, V.D. Timofeev, N.V. Sviridov, I.B. Andryenko.
State Medical University, Donetsk
Resume. The work is a study of the course of the wound process when using the enterosorbent "Atoxyl" in patients with diabetic foot syndrome.
Keywords: diabetic foot syndrome, enterosorbent, treatment
Diabetic foot syndrome is a serious complication of diabetes. This disease often leads to disability. It is known that the risk of developing gangrene in these patients is 10–15 times higher than in people who do not suffer from diabetes. Approximately 50% patients with diabetes have once undergone surgery [2, 3, 4].
As a result of impaired blood supply and innervation, diabetes leads to a delay in healing processes and a high risk of wound infection. Poor wound healing occurs in 50% cases, and the risk of infection is 5 times higher. Consequently, surgical treatment of purulent-necrotic lesions in diabetic foot syndrome is a difficult task [5, 6, 7].
Despite the achievements of modern medicine, the level of high limb amputations remains high and ranges from 40 to 50% [V.B. Kuramov, N.B. Toothless]. An important task of surgical treatment of complicated forms of the diabetic foot is to reduce mortality from purulent-septic complications and preserve the supporting function of the foot.
The purpose of the work was to study the course of the wound process when using the enterosorbent "Atoxyl" in patients with diabetic foot syndrome.
Materials and methods. A center for the treatment of patients with diabetic foot syndrome operates in the clinic of surgical diseases of the FPO No. 2 of DonSMU. Over the past 6 months, we have treated 37 patients with this pathology aged 52 to 76 years (15 men, 22 women). Of them, 12 patients with trophic ulcers; after opening phlegmon – 4; after resection of the foot - 9; after the exarticulation of the fingers - 12. The study of the course of the wound process was carried out by cytological examination of swabs from the wound exudate or an impression from the bottom of the wound within 1 to 7 days of postoperative intervention. The analysis of the exudate from the wound allowed us to judge the course of the wound process and the influence of the enterosorbent in the complex treatment of diabetic foot syndrome. After fixation, smears and prints were stained according to Romanovsky-Giemse. Smears and prints were subjected to qualitative and quantitative studies, and at the same time, a microscopic study of the microflora in smears and prints was conducted in dynamics when using an enterosorbent.
General clinical and biochemical analyzes of blood and urine were performed on patients, ultrasound dopplerography was performed to study blood flow, volume blood flow was studied on the Logic-5 device. To the complex treatment described in one of our reports [1], we added the drug "Atoxyl", which is an enterosorbent produced by CJSC "Lviv Pharmaceutical Factory" registration number UA/2616/01/01, which belongs to silicon ultrahigh-dispersion enterosorbents of the IV generation. This drug was used by us in the treatment of purulent-necrotic wounds as one of the stages of wound preparation before closing the wound defect with an amniotic membrane. For small defects, the drug in the amount of 3–5 g was applied to the wound and covered with a dry bandage. Dressings were made every other day. With large defects on the foot, which appeared after the opening of phlegmon, resection of the foot, we used an absorbent bandage, which is several layers of gauze filled with an enterosorbent. After opening the phlegmon and resection of the foot according to Chopar, Sharp or at the level of the Lisfranc joint, after appropriate treatment with the removal of purulent-necrotic foci to healthy tissues, "Atoxyl" was placed in the wound in the above-described bandage from the first to second day. Dressings were made daily with washing of the wound with solutions of antiseptics.
Results and discussions. The postoperative period in all patients was different and depended on the level and degree of foot damage (localization, depth of purulent-necrotic processes, etc.). The main criterion for evaluating the effectiveness of treatment was the state of the cellular composition of the separated wound in the dynamics during treatment.
A day after surgery, 23 patients were cytologically diagnosed with signs of acute staphylococcal infection (++++) with the death and dystrophy of neutrophilic leukocytes, incomplete phagocytosis up to 11%, with the presence of 15–20 staphylococci per p/zr. In 11 patients, only single staphylococci were determined among the cellular elements of the blood or there were no microbes at all.
5–7 days after the operation, under the influence of complex and local treatment, staphylococcal microflora disappeared and phagocytosis was completed. At the same time, the number of preserved neutrophilic leukocytes increased in the wound exudate. In the rest of the patients, the exudate from the wound was sterile according to cytological data.
Only in three patients in whom "Atoxyl" was used, 2–3 days after the operation, a moderately expressed staphylococcal wound infection (++) with incomplete phagocytosis was observed.
Quantitative cytological studies of the cells of the wound exudate obtained from the wound indicated, in general, relatively pronounced inflammation at the bottom of the wound, which was equally pronounced after the first or second day after the operation.
The differences in the dynamics consisted in a decrease in the number of dystrophically altered neutrophils two days after the operation compared to the first days. When comparing the reaction of neutrophils in the exudate from the wound obtained a day after the operation, a slightly more pronounced inflammatory reaction was noted if "Atoxyl" was not used (24–26 in p./sp.) compared to wounds where "Atoxyl" was used (10–15 p./sp.). At the same time, 1–2 days after the operation, the percentage of connective tissue cells from the separated wound was higher in wounds with the use of "Atoxyl" than in wounds without its use.
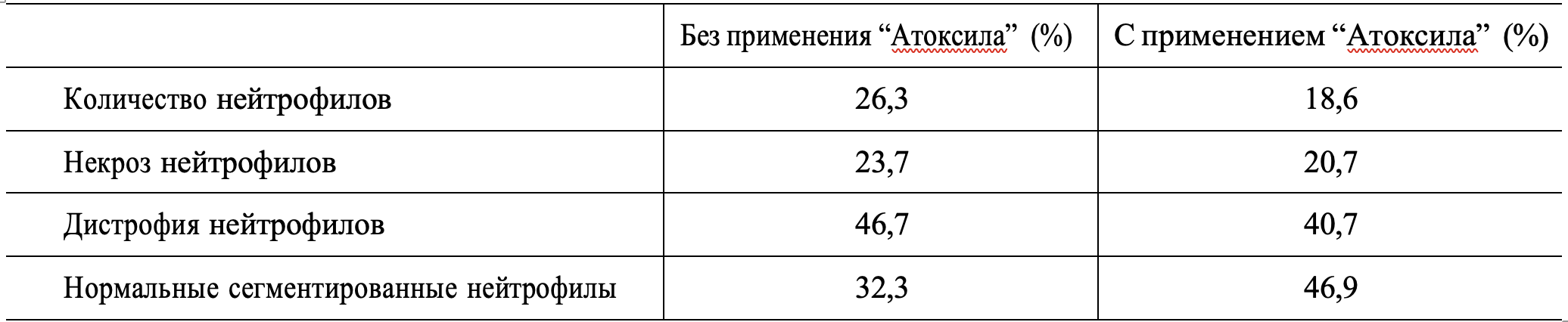
2–3 days after the operation, in wounds without the use of enterosorbent, the inflammatory reaction was at a higher level (26.3% of neutrophils per p/sp., necrosis - 23.7%, neutrophil dystrophy - 46.4%) than in wounds with the use of "Atoxyl" (18.6% of neutrophils per p/sp., necrosis - 20.7%, dystrophy - 40.7%), and the number of normal segmented neutrophils was significantly less (32.3–46.9%), which corresponded to the data noted above during the wound process in the absence of treatment or when using this sorbent.
The course of the wound process after 2-3 days is presented in the table:
The obtained cytological data allow us to conclude that the enterosorbent "Atoxyl" used in complex treatment improves wound cleansing, which contributes to the reduction of wound preparation time for plastic surgery. In the same cases when the enterosorbent was not used, suppuration and the development of the necrotic process in the wound were noted. 2–3 days after the operation, a wound infection was detected in 12 and 25 patients, respectively, with the presence of staphylococcus (+) and Gram-positive bacillus (+) in the wounds when Atoxyl was used and without its use. The infection intensified the necrotic-dystrophic process in these patients. 5–7 days after the operation, wound infection due to staphylococci was noted in 12 patients. However, the infection was stopped by the introduction of antibiotics. The marked wound infection did not significantly affect the proliferation of connective tissue cells, and the inflammatory reaction was moderate or weak.
Based on the results of the study, the terms of surgical interventions were determined. Thus, in the group of patients without the use of "Atoxyl", the possibility of performing the specified interventions arose within 20–22 days (21 ± 3 days on average). In the group of patients who received "Atoxyl", the possibility of performing the specified interventions arose within 14–16 days (on average 15 ± 3 days).
Conclusions.
- Thus, there is a difference in the degree of wound infection with and without the use of Atoxyl.
- The obtained data testify to the positive effect of the enterosorbent "Atoxyl" on the course of the wound process, in particular, when it is prepared for the closure of the amniotic membrane. This made it possible to reduce the time of wound preparation from 20-22 days to 14-16 days.
Literature
- Antonyuk S.M., Sviridov N.V., Popandopulo A.G. etc. Features of surgical treatment of patients with complicated forms of diabetic foot syndrome // Clinical Surgery - No. 10. - P. 36-39.
- Bregovsky V.B. Scientifically based standards of diagnosis and treatment of purulent-necrotic complications of the diabetic foot syndrome in ambulatory-policlinic conditions // Standards of diagnostics and treatment in purulent surgery. Scientific and practical materials. conference, Moscow, Oct. 23-24 2001.
- Gostischev V.K., Afanasyev A.N. Standards of medical and diagnostic measures in patients with diabetic osteoarthropathy and purulent-necrotic lesions of the feet // Standards of diagnostics and treatment in purulent surgery. Scientific and practical materials. conference, Moscow, Oct. 23-24
- V.V. Hrubnyk, V.V. Hot, A.S. Pylypenko, E.A. Antsypovych. A modern approach to the treatment of complicated diabetic angiopathy of the lower extremities // Clinical Surgery. – – No. 7. – P. 11-13.
- Dedov I.I. Diabetes mellitus - problem XXI // Doctor. – – No. 1. – P. 4-5.
- Lyapis M.O., Gerasymchuk P.O. Justification of the early use of autodermoplasty in the treatment of wounds in patients with diabetic foot syndrome //Clin. Surgery. – – No. 8. – P. 30-32.
- Shor N.A., Zeleny I.I. Indications and selection of the level of amputation of the lower extremity due to diabetic angiopathy with purulent-necrotic lesions of the tissues of the foot // Klin. surgery. – – No. 8. – P. 47-49.