Acetonemic syndrome in children: tactical steps of a practicing doctor
V.V. Berezhnoi, V.V. Korneva, V.G. Kozachuk, L.V. Kurylo, E.A. Boyarskaya, M.A. Kapychyna, A.V. Shoemaker
National medical academy of postgraduate education named after P.L. Shupyka, Kyiv City Children's Clinical Hospital No. 1
Resume. The article offers criteria for an early diagnosis of acetonemic syndrome in children who allow family doctors and pediatricians to timely diagnose primary acetonemic syndrome (syndrome cyclic vomiting — CVS): detailing of family history; detailing the history of the child's illness and life; Adequate assessment of leading symptoms in the non-seizure period. Knowledge of these clinical and anamnestic indicators will make it possible to timely and adequately start the initial therapy of acetonemic syndrome in children (both primary and secondary) with a highly effective rehydration agent - Regidron Optim in combination with a 4th generation enterosorbent - the drug Atoxyl.
Keywords: acetonemic syndrome, children, rehydration therapy, Regidron Optim, enterosorption, Atoxyl.
Introduction
Acetonemic syndrome of children (ASD) is one of the most common diseases of childhood, which is manifested by stereotyped repeated episodes of vomiting, alternating with periods of complete well-being.
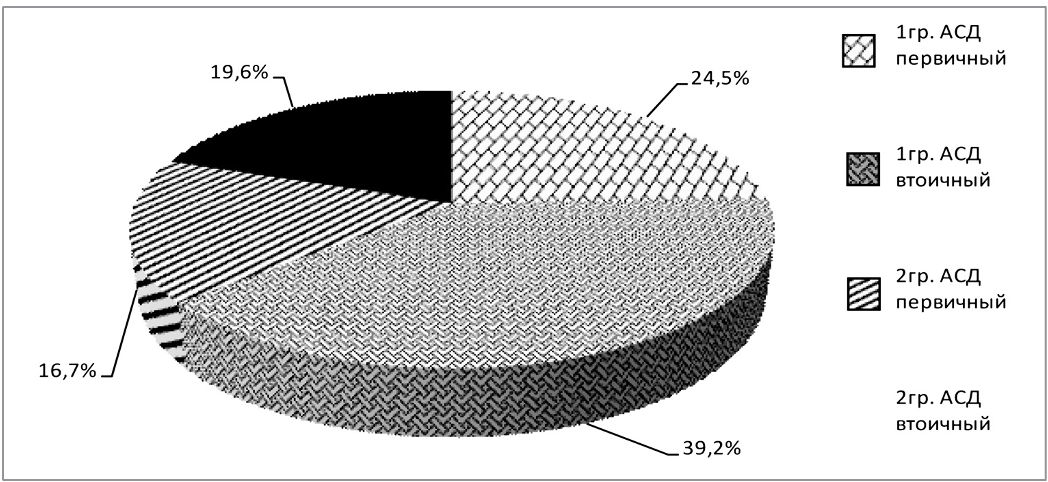
Most domestic pediatricians distinguish two types of ASD — primary and secondary [1,4,6,7].
Primary ASD occurs in children with a neuro-arthritic constitutional anomaly (uric acid diathesis) and is characterized by a violation of purine metabolism with excessive production of uric acid and its precursors, instability of carbohydrate and lipid metabolism (with a tendency to ketosis), lability of the mediator functions of the nervous system, which determine the peculiarities of its reactions. ASD occurs mainly in children aged 2 to 10 years and is manifested by hyperuricemia and periodic metabolic (acetonemic) crises with the development of hyperketonemia, acetonuria, and acidosis. But in recent years, such conditions are increasingly common in adolescence.
Secondary ASD most often occurs with: infectious toxicosis; combined pathology of the gastrointestinal tract, accompanied by symptoms of intoxication, cholestasis; toxic liver damage; when intestinal microflora is disturbed. The cause of secondary ASD can also be: starvation, decompensated diabetes, hyperinsulinism, insulin hypoglycemia, glycogen disease, thyrotoxicosis, traumatic brain injury, brain tumor in the region of the Turkish saddle, Itsenko-Cushing disease, leukemia, hemolytic anemia, and other conditions. The clinical picture of the acetonemic syndrome in such cases is determined by the main disease, on which ketonemia is superimposed [6].
Literary data on the prevalence of primary and secondary ASD are contradictory. Yes, A.S. Senatorova, E.V. Osypenko (2007) [12] believe that secondary ASD occurs twice as often in children as primary ASD. Similar data are given by L.V. Kvashnina N.B. Evgrafova (2003) [6]. I. Booth, R. Cunha Ferreira, JF Desjeux et al. (1992) [16] in their research showed that primary ASD in pediatrics occurs 2.4 times more often than secondary situational acetonemic syndrome.
Features of ASD are high lability of metabolic and water-electrolyte changes, relationships with background conditions and vegetative syndromes inherent in children of different age groups.
The metabolic basis of the development of ketoacidosis is increased lipolysis, which leads to the entry of a large amount of fatty acids into the liver. Limited opportunities for utilization of lipolysis products lead to excessive formation of ketone bodies - acetone, acetoacetic and beta-oxybutyric acids, which irritate the mucous membrane of the alimentary canal, which causes abdominal pain and vomiting.
Ketone bodies also cause the development of metabolic acidosis, which leads to: disruption of hemodynamics (peripheral vasospasm) and the resulting relative hypovolemia, which is further aggravated by vomiting; drug-like effect on the central nervous system. Ketone bodies provoke compensatory hyperventilation (hypercapnia), the smell of acetone appears when breathing, and ketone bodies are found in the urine. As a result, a typical picture of the acetonemic syndrome is formed [11].
The development and course of ASD are aggravated by: nervous-arthritic diathesis; liver diseases (disruption of lipolysis); pathology of the tubular system of the kidneys (COS violation); diseases of the pancreas (functional insulin deficiency, disorders of exocrine function); changes in the lungs (participation in compensatory dyspnea). Vomiting that occurs in these conditions, perspiratory fluid losses due to shortness of breath lead to pronounced disturbances of the electrolyte balance in children [5,6].
It should be noted that in the last decade, most researchers of primary ASD treat this condition as "cyclic vomiting syndrome" (CVS). Most pediatricians and family doctors are aware of the commonality in most of the mechanisms of etiology and pathogenesis leading to the clinical symptoms of these conditions. The introduction of the protocol "Syndrome of cyclic vomiting" (order of the Ministry of Health of Ukraine No. 438 of 26.05.2010 "Protocols for the diagnosis and treatment of diseases of the digestive organs in children") will focus pediatricians and family doctors on the analysis of family history, in particular, the relationship with migraine and other pathogenetically similar conditions [11,13]. However, a number of protocol approaches in the treatment of ASD, especially at the outpatient and outpatient stage, during 2010–2011. were criticized by the medical community. The new version of the Protocols will bring the modern etiopathogenetic approaches in the treatment of ASD as close as possible to the real possibilities of treatment of this condition in Ukraine.
The long-term experience of the pediatric service in stopping ASD, especially at the outpatient clinic stage, testifies to the high effectiveness of oral rehydration in the majority of patients with ASD [1,12,15].
The expressiveness of metabolic and water-electrolyte changes, the lability of these processes motivates pediatricians to search for optimal methods of treatment of ASD, available both for outpatient and outpatient practice, and for hospital practice.
Such methods include the use of oral rehydration therapy in combination with modern enterosorbents in the complex treatment of ASD. Such a tactic will allow you to quickly stop the main symptoms of ASD — metabolic and water-electrolyte changes.
For many years, the undisputed leader in oral rehydration therapy was the drug "Regidron", and since 2010, its pediatric form - Regidron Optim - has been widely used in Ukraine.
As shown by the works of a number of authors, despite its short presence on the pharmaceutical market of Ukraine, Regidron Optim is quite widely used as a rehydration agent in the practice of pediatricians and family doctors [1].
Rehydron Optim (REHYDRON OPTIM) Orion is a preparation, the composition of which per 1 liter of solution includes: sodium chloride - 2.60 g (44.444 mmol/l), sodium citrate - 2.90 g (29.565 mmol/l), potassium chloride - 1.5 g (20.134 mmol/l), anhydrous glucose - 13.5 g (74.92 mmol/l). Excipients: acesulfame potassium, lemon flavoring. The osmolarity of the Rehydron Optim solution is 245 mosm/l. The composition of Regidron Optimpolnosti solution fully complies with international standards, in particular with the recommendations of the European Society of Pediatric Gastroenterology and Nutrition (ESPGAN).
The form of release is also convenient - 1 sachet per 500 ml of the finished solution. The package contains 6 sachets, from which you can prepare 3 liters of rehydration solution. This amount of solution in most cases is the optimal course dose for children of early age. It should be noted that lemon flavoring is a non-allergenic component of the solution. The optimal age to start taking this drug is from birth. In case of nausea and vomiting, Regidron Optim should be taken chilled in small repeated doses. The recommended daily dose per 10 kg of body weight is at least 0.5 l of Regidron Optim solution, which is equal to 1 sachet (information taken from the Compendium it-apharm.ru 2009–2010). If necessary, this dose is increased one and a half to two times.
It should be noted that rehydration therapy for ASD, according to the recommendations of many researchers, is prescribed individually depending on age, body weight and degree of dehydration. In the first 6 hours of treatment, the volume of oral salt solutions (ORS) is 20–30 ml/kg of body weight. The total volume of fluid during the first 6 hours of rehydration therapy is in most cases 30–40 ml/kg, and if necessary, up to 60 ml/kg [11,12].
The daily volume of fluid in the first 1–3 days of treatment is from 60 ml/kg to 100 ml/kg of the child's body weight. Out of this amount of ODS, there should be no less than 70%. In addition to this, it is possible to use other liquids (dried fruit decoctions, boiled water, degassed alkaline mineral water) [4,7]. If necessary, solutions should be taken in small amounts (a teaspoon or a tablespoon depending on age) every 5–15 minutes, then the single dose can be gradually increased.
In addition to oral rehydration therapy, which is expediently started even before the development of vomiting, in particular, when the child develops lethargy, loss of appetite, it is very important to connect enterosorbents during the same period [7,14].
The main purpose of prescribing enterosorbents, both in the prodromal period of ASD and in the period of an attack, is to carry out detoxification and improve the evacuation function of the stomach.
Such enterosorbents include Atoxyl, a drug of the new, 4th, generation of sorbents (Silica "Orisyl®", produced by "Orisyl" LLC, which has passed the test for compliance with FDA standards and the USA Pharmacopoeia according to USP29 - NF24 monograph tests) [2,3,8].
The main feature of the drug Atoxyl (ultra-high-dispersity non-porous silicon sorbent) is its protein sorption ability, thanks to which binding, inactivation and removal from the body of exo- and endotoxins, allergens, antigens, degradation products of necrotic tissues and other harmful substances of protein origin occurs. These features of the drug Atoxyl provide a powerful detoxification effect.
In comparison with other sorbents (coal, organic polymers), Atoxyl has the highest active surface area of sorption, about 400 m2/g. Thanks to these properties, Atoxyl provides a rapid reduction of endogenous intoxication already from the first administration of the drug. Due to its non-porous nature, the peak activity of the drug is observed already 4 minutes after its administration [2,9,10].
In cases of secondary ASD arising on the background of viral diarrhea or OKI, the therapeutic effect of Atoxyl is also due to its ability to bind microorganisms and viruses with an activity of up to 1010 microbial bodies per 1 g. Thanks to this, there is adsorption of microbes and viruses, bacteriostatic and, indirectly, bactericidal action, inhibition of the invasion of pathogenic microflora through the mucous membrane of the gastrointestinal tract, which prevents the development endotoxicosis, quickly eliminates the main symptoms of the disease [3,9,10].
The drug Atoxyl has a high safety profile, therefore it is recommended for children from 1 year of age. Unlike coal sorbents, it does not injure the gastric mucosa and is completely excreted from the body. It is also hypoallergenic. Compared to existing sorbents, Atoxyl has significantly better organoleptic properties. The drug is easily accepted by children and adults [3,8].
Recommended doses of Atoxyl in children: 1–2 years — single dose — 1 g of the drug, average daily dose — 2 g; 2–4 years, single dose — 1 g, average daily dose — 3 g; 4–7 years — single dose — 2 g, average daily dose — 4 g;
Table 1
Age composition of examined patients

Fig.1. Variants of acetonemic syndrome in examined children 7–12 years old — single dose — 2 g, average daily dose — 5–6 g; children older than 12 years — single dose — 4 g, average daily dose — up to 8 g.
All of the above motivated us to introduce and study the effectiveness of Regidron Optim and Atoxyl in the treatment of ASD. The work was carried out on the basis of the Kyiv City Children's Clinical Hospital No. 1 (head doctor - Yu.A. Kozhara), which is the clinical base of the Department of Pediatrics No. 2 of the NMAPO named after P.L. Shupyka (the head of the department is Professor V.V. Berezhnoi). The research was conducted in 2011–2012.
Materials and research methods
In the department of gastroenterology, as well as in patients of the consulting clinic, the drugs Atoxyl and Regidron Optim were used in the complex therapy of 65 children with acetonemic syndrome (group 1). In 37 patients with ASD, alkaline drink or other oral solutions were used in therapy, Atoxyl enterosorbent was not prescribed (group 2). Diagnosis of acetonemia was carried out using CITOLAB K (ketones) strips from the Farmasco company.
The age of patients in all groups was from 1 year to 14 years (Table 1). The division by gender and age in both groups was relatively equivalent.
Secondary ASD was registered in 60 children of groups 1 and 2 with infrequent (absence of cyclicity) or one-time episodes of acetonemic vomiting. This syndrome arose against the background of: ARVI with hyperthermic syndrome, at the onset of viral diarrhea; functional dyspepsia, DZVP, during deworming, during food allergic reactions. In such cases, ASD was defined as the main disease on which ketonemia was superimposed.
The group of primary ASD included 42 patients with manifestations of urinary salt (uric acid) diathesis. In these children, in 80% cases, there were changes in the study of salt transport, confirming the diagnosis.
Research results and their discussion
In children with primary acetonemic syndrome, cyclicity of vomiting with satisfactory interictal periods was noted. Paroxysmal migraine-like headaches prevailed in 34 patients of groups 1 and 2 with primary ASD (80%), and the age of these patients was over 9 years. These same children had episodes of paroxysmal autonomic failure. A detailed anamnestic spectrum of complaints and features of symptoms in the non-epileptic period in patients with primary ASD (CVS) are presented in Figure 2.
Taking into account the above data, according to the Rome III criteria, the diagnosis of "Cyclic Vomiting Syndrome" (CVS) should have been more valid in all examinees who were included in the group of primary ASD.
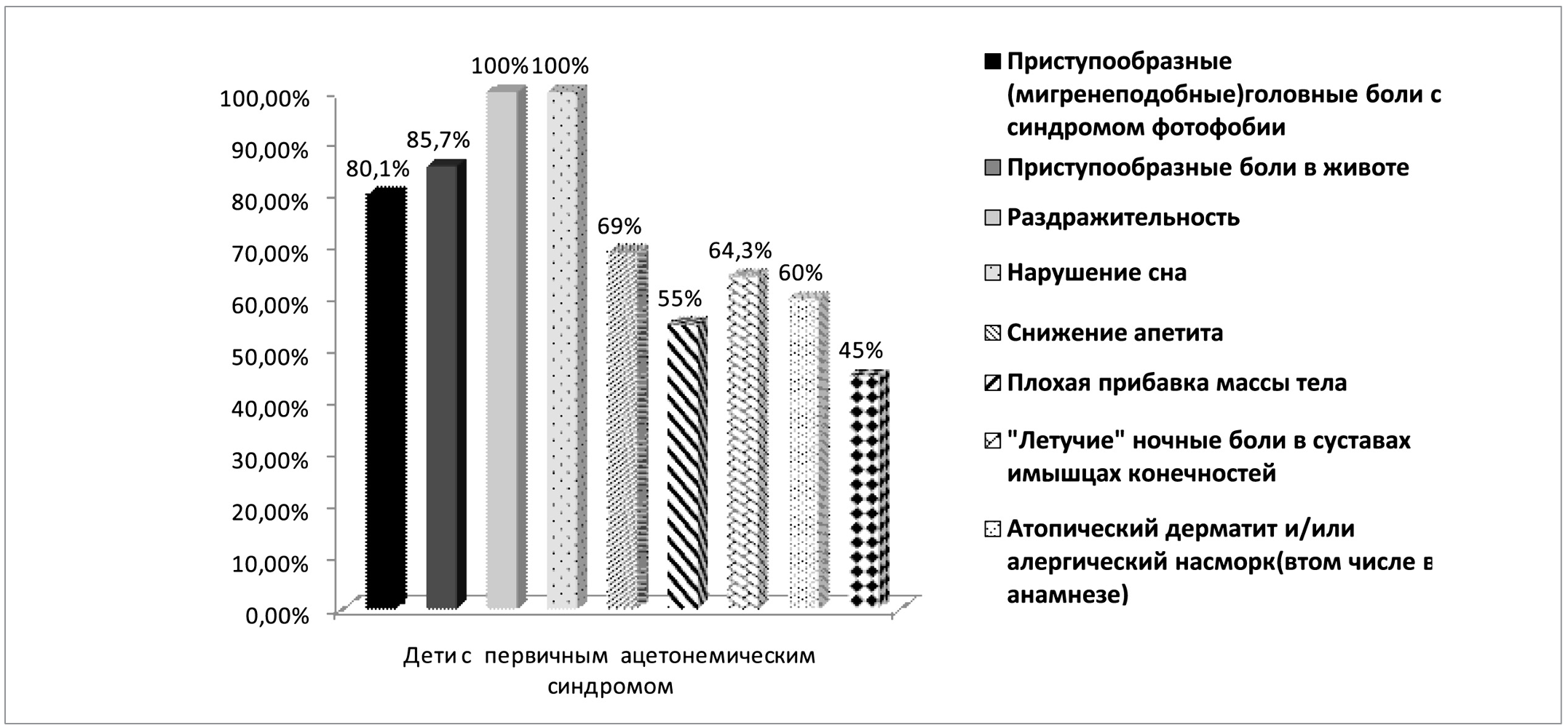
Fig.2. Clinical symptoms of the non-epileptic period in patients with primary ASD (CVS).
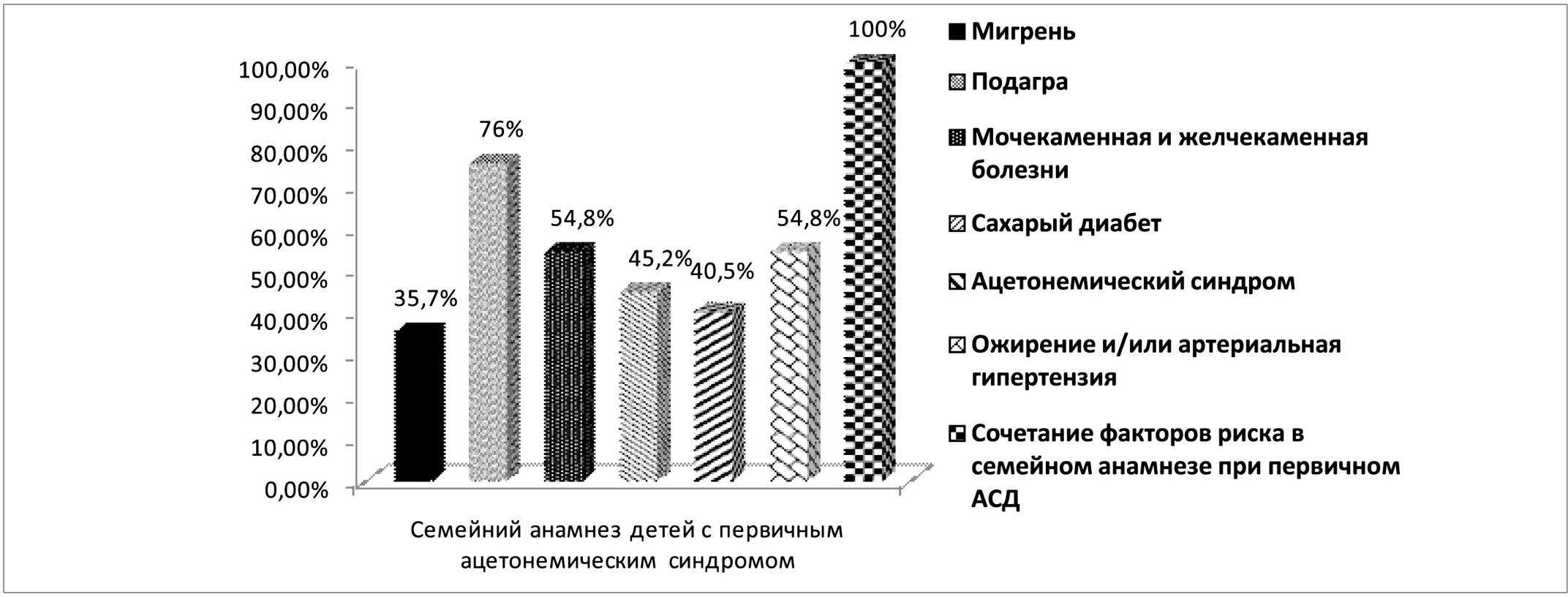
Rice. 3. Peculiarities of the family history of children with primary acetonemic syndrome (% occurrence in family members)
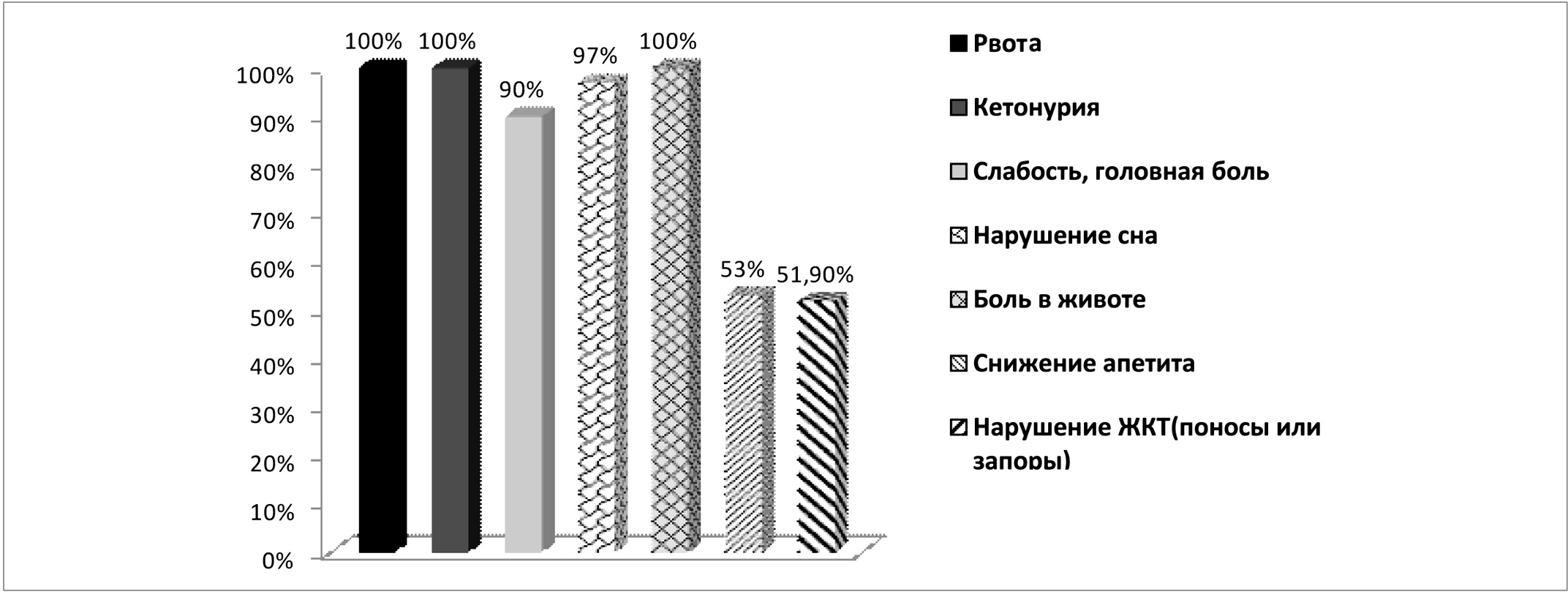
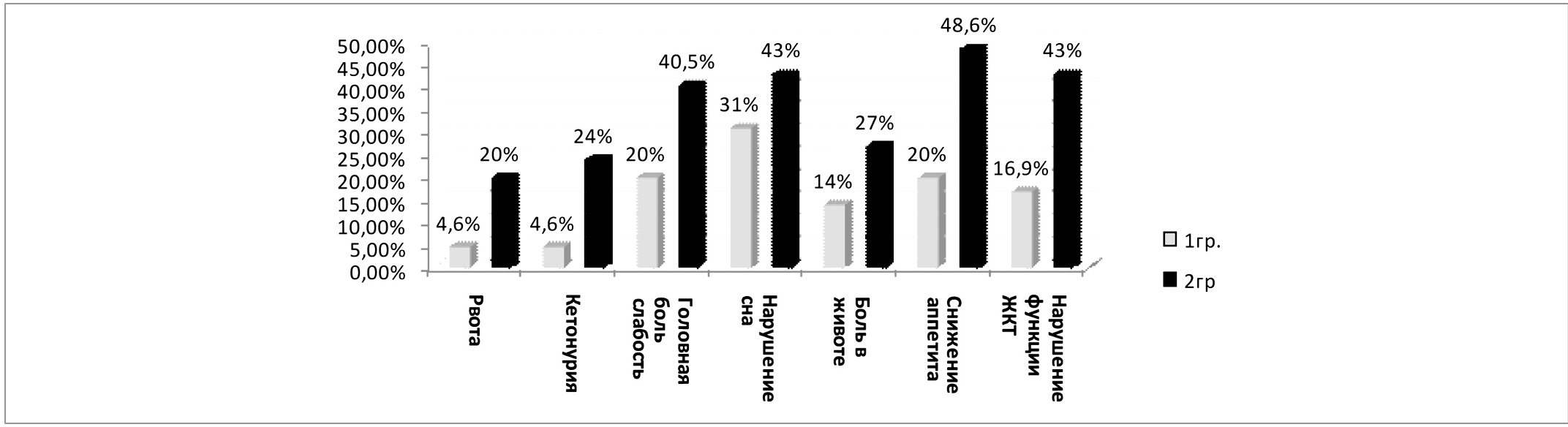
Rice. 4. Complaints in ASD at the time of onset of the disease
Table 2
Biochemical indicators in examined children at the beginning of the onset of acetonemic syndrome

Given that such changes are familial, we analyzed in detail the family anamnesis in the primary ASD group (42 patients in total). Features of the family history of children with primary acetonemic syndrome are presented in Figure 3.
As can be seen from the data in Figure 3, risk factors for the development of ASD were present in all children with primary ASD, which is one of the leading criteria for early diagnosis of cyclic vomiting syndrome (CVS) [11,12,13].
The data presented in Figures 2 and 3 should be carefully analyzed by family doctors and pediatricians for the purpose of early diagnosis of primary ASD. You should also pay attention to family risk groups ("risk factors") for the development of ASD with the corresponding regimen, dietary and, if necessary, medication recommendations.
Complaints of all examined children at the time of admission are presented in Figure 4.
It should be noted that the paraclinical indicators upon admission to the hospital or the beginning of outpatient treatment in groups 1 and 2 were similar and did not differ statistically.
The results of the study of biochemical parameters in children of all groups at the beginning of the acetonemic syndrome are presented in table 2.
As can be seen from table 2, at the beginning of the disease in children of all groups, a decrease in the level of sodium, potassium, and calcium in the blood plasma was noted, and an increase in the hematocrit level was noted. This indicates electrolyte losses and BCC changes. Such conditions are the basis both for carrying out rehydration therapy and for prescribing detoxification-oriented drugs.
Rice. 5. Dynamics of the main clinical symptoms during treatment (by the 5th day of therapy)
Table 3
Dynamics of blood electrolyte indicators in children with acetonemic syndrome (5th day of treatment)

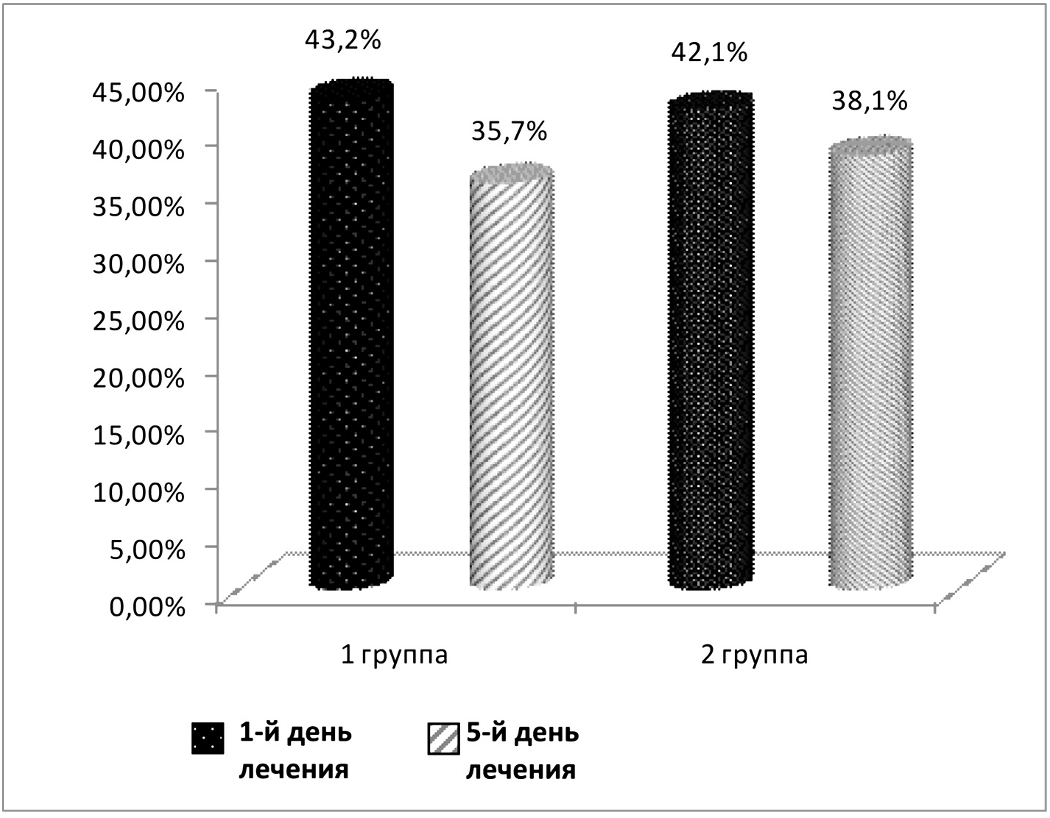
Rice. 6. Dynamics of hematocrit indicators in examined children during treatment (1 and 5 days of treatment)
Rehydration therapy for children in group 1 was carried out with Regidron Optim solution, in group 2 - with other rehydration agents. The children of group 1 were also immediately prescribed the 4th generation enterosorbent Atoxyl.
The duration of rehydration therapy in combination with the use of enterosorbent Atoxyl in 1 group was up to 3 days in 70.8% (46 children). By day 5, all children in this group did not need rehydration therapy.
In the 2nd group, rehydration therapy was carried out for 3 days in 56.7% (21 children), and by the 5th day of treatment, the effect was achieved in 75.7% (28 children) examined.
Most of the children (80% examined) were given a cleansing enema with 1% baking soda solution 1–2 times a day during the first three days of treatment. If necessary, antiemetic and antispasmodic drugs were administered symptomatically. In the first days of treatment, the children received individual fractional feeding (pounded soups, warm sweet drinks, crackers). In the future, diet therapy also corresponded to the protocol recommendations.
All patients of group 1 tolerated well the combined therapy with Regidron Optim and Atoxyl. The absence of the need to prescribe infusion therapy in this group of patients speaks of the effectiveness of the indicated therapy.
In group 2, the rate of infusion interventions was 32.4% (12 cases), and this treatment was carried out both in primary and secondary ASD.
The dynamics of the main clinical symptoms during treatment (in particular, by the 5th day of therapy) is presented in Figure 5.
As can be seen from the data in Figure 5, the positive dynamics in group 1 was significantly ahead of the similar indicators of patients in group 2 (in all cases, p<0.05).
The dynamics of examination of patients during treatment is presented in Table 3 and Figure 6.
As can be seen from the data in Table 3 and Figure 6, indicators of electrolyte exchange and hematocrit in the course of treatment tended to normalize in all examined patients. However, by the 5th day of therapy, this positive dynamic is more clearly visible in patients of the 1st group compared to the 2nd group.
Taking into account the positive dynamics of the disease, 100% children of group 1 were discharged by the 6th day of hospital stay. The average length of hospital stay for children in group 2 was 7.9 bed-days.
Conclusions
Thus, for medical workers and parents, it is very important to determine the nature of ASD (primary or secondary), which will allow a differentiated approach to the treatment and prevention of these conditions. To determine the type of acetonemic syndrome in children, it is very important to take a correct family history and detail the clinical features of the interictal period.
Family doctors and pediatricians should pay special attention to the presence of so-called "risk factors" in the family: migraine, urolithiasis or gallstone disease, gout, diabetes mellitus, acetonemic syndrome in childhood in family members, obesity and/or arterial hypertension. Because the complete or even partial combination of these "risk factors" in the family history of patients with ASD is one of the criteria for early diagnosis of primary acetonemic syndrome (CVS).
For the timely diagnosis of primary ASD, it is very important to pay attention to the leading manifestations of the non-epileptic period and anamnestic data in the child: paroxysmal (migraine-like) headaches; paroxysmal abdominal pain; irritability, sleep disturbance; decreased appetite, poor weight gain; "volatile" night pains in the joints and muscles of the limbs; tendency to atopic dermatitis and/or allergic rhinitis, enuresis and/or logoneurosis (including history).
According to our data, the presence of one or another of the specified manifestations of the non-convulsive period and features of the anamnesis, including family history, was noted in all patients with primary acetonemic syndrome. Moreover, in more than 80% children, a combination of "risk factors" was registered in three or more positions, and in one third of patients, their 100% combination was revealed.
In the treatment of acetonemic syndrome in children (both in the prodromal and in the acute period), high efficiency is achieved with the early appointment of rehydration therapy using the drug Regidron Optim in combination with the enterosorbent of the 4th generation - the drug Atoxyl.
The proposed approach to the problem of acetonemic syndrome in children, which will allow family doctors and pediatricians to timely suspect or diagnose primary acetonemic syndrome in children (cyclic vomiting syndrome — CVS), includes: detailed family history; detailing the child's illness and life history (according to specified criteria); adequate assessment of leading symptoms in the non-epileptic period.
Knowledge of these clinical and anamnestic indicators will allow timely and adequate starting therapy of acetonemic syndrome in children (both primary and secondary) with a highly effective rehydration agent (Regidron Optim) in combination with a 4th generation enterosorbent (Atoxyl).
The totality of such approaches will enable family doctors and pediatricians to optimize the therapy of such a common condition as acetonemic syndrome in children and improve the quality of life of these patients.
LITERATURE
- Acetonemic syndrome in children — opportunities for optimization of therapy / V.V. Korneva, V.V. Kozachuk, L.G. Kurylo [and others] // Current gastroenterol. — 2011. — No. 2. — P. 45-48.
- Bondarev, E. V. Use of enterosorbents in medical practice [Electronic resource] / E. V. Bondarev, S. Yu. Shtrygol, S. B. Dyryavy. — Kh.: National Pharmaceutical University.— Mode of access: http://www.provisor.com.ua. — Title from the screen.
- Effectiveness of enterosorption therapy in the complex treatment of ascariasis in children: inform. letter. / V. V. Berezhny, T. V. Marushko, V. V. Korneva [et al.]. — K., — 4 p.
- Zubarenko A. V. Dysmetabolic nephropathy in pediatric practice. Communication / A. V. Zubarenko, T. V. Stoeva // Zdorovyerebenko. — 2009. — No. 4 (19). - pp. 22-25.
- Kazak S. S. Diagnosis and diet therapy of acetonemic syndrome in children / S. S. Kazak, G. V. Beketova // Medicines of Ukraine. — —№ 1. — pp. 83—86.
- Kvashnina L. V. Neuro-arthritic constitutional anomaly, disorders of purine metabolism and acetonemic syndrome in children / L. V. Kvashnina, N. B. Evgrafova // Doctor. — — No. 3. — P. 79-82.
- Kurylo L. V. Acetonemic syndrome: a disease or a way of life? / L. V. Kurylo // Health of Ukraine. — — No. 10. — P. 34-35.
- Nadraga O. B. The effectiveness of the use of the sorbent "Atoxil" in the complex treatment of rotavirus gastroenteritis in young children / O. B. Nadraga, G. O. Lytvyn, N. M. Potsiluyko // Sovrem. pediatry. — 2011. — No. 2. —P. 138—141.
- Evaluation of the effectiveness of the enterosorbent Atoxyl in the complex treatment of ascariasis in children / V.V. Korneva, L.V. Kurylo, V.G. Kozachuk [and others]// Sovr. pediatrics — — No. 3. — P. 62-65.
- Paliy I.G. Contemporary view on the problem of enterosorption: selection of the optimal drug / I.G. Paliy, I.A. Reznychenko // Nov. medicine and pharmacy. — — No. 11 (217). — P. 15-17.
- Yu. S. Sapa Syndrome of cyclic acetonemic vomiting / Yu. S. Sapa [Electronic resource]. — Access mode: http://www.rekicen.ru/php/content.php?group=1&id=422. — Title from the screen.
- Senatorova A. S. Acetonemic syndrome in children / A. S. Senatorova, E. V. Osypenko // Health of the child. — — No. 5 (8). - pp. 42-46.
- Cyclic vomiting syndrome. Protocols for the diagnosis and treatment of digestive diseases in children: Order of the Ministry of Health of Ukraine No. 438 of May 2010 [Electronic document]. — Access mode: http://www.moz.gov.ua. — Screen name.
- Apical effect of diosmectite on damage to the intestinal barrier induced by basal tumor necrosis factor / Mahraoui, M. Heyman, O. Plique [et al.] // Gut. —1997. — Vol. 40. — P. 339—343.
- Kim Y. Reduced osmolarity oral rehydration solution for treating dehydration due to diarrhea in children: systematic review / SY Kim, P. Garner // BMJ. —2001. — Vol. 323. - P. 81-85.
- Recommendations for composition of oral rehydration solution from the children of Report of an ESPGAN working group
- Booth, R. Cunha Ferreira, JF Desjeux [et al.] // J. Pediatr. Gastroenterol. Nutr. — 1992. — Vol. 14. — P. 113—115.