Application of sorption methods in liver disease associated with intestinal dysbacteriosis in young children
UDC 616.36-053.36:615.246.2
O.H. Shadrin, N.F. Chernega
State Institution "Institute of Pediatrics, Obstetrics and Gynecology of the National Academy of Medical Sciences of Ukraine", Kyiv
Resume. The article presents the results of the effectiveness of the drug "Atoxil" in the complex treatment of young children with liver damage associated with intestinal dysbiosis.
Key words: children early age, disease liver, Atoxil.
Introduction
Liver damage in young children is an extremely urgent problem, which is due, first of all, to the low effectiveness of treatment and the rapid progression of fibrotic changes in this age category.
The principle of treatment of liver diseases involves two main directions: etiotropic and pathogenetic therapy. Etiotropic therapy is used for viral lesions and is strictly justified and standardized. Given its limited use and low effectiveness in the treatment of young children, an important direction of treatment is pathogenetic.
The hepatobiliary system is the main connecting link between the gastrointestinal tract (GI) and the internal environment of the body. The GI tract is the first functional barrier that ensures the absorption and concentration of not only necessary but also harmful substances, which include the waste products of the intestinal microflora. Dysbiotic changes in the intestine are among the adverse factors of liver damage [3].
Normal microflora in the body performs a number of important functions, including the synthesis of vitamins (B1, B2, B6, K, folic, nicotinic acid, etc.) and participation in digestive processes. Food components are broken down by a wide range of bacterial enzymes to oligomers, which in turn are fermented to short-chain fatty acids, organic acids and other products. The final components of hydrolysis provide trophism of the intestinal mucosa, increase its energy potential and stimulate motility. An important function of the intestinal microflora is participation in the activation of local and general immune reactions. The intestinal mucosa, having its own lymphoid system, is one of the most significant components of the immune system of the macroorganism. Normal intestinal microflora participates in the activation of immune reactions and the formation of immune tolerance of the macroorganism.
Imbalance of intestinal microflora leads to an increase in the proportion of potentially pathogenic gram-negative bacteria that produce toxic metabolites. Using protein and its hydrolysis products as a food substrate, pathogenic microflora causes putrefactive processes, the final metabolites of which are ammonia, aromatic amino acids, sulfites, endogenous toxins. The products of such metabolism contribute to inflammation of the mucous membrane, diarrhea, impaired parietal digestion, and increased gas formation. Endotoxins of pathogenic bacteria accumulated in the intestinal lumen penetrate through the intestinal mucosa into the circulatory system and portal vein and cause damage to hepatocytes. Anaerobic gram-negative bacteria facultatively release up to 90% of all endotoxins that damage cell membranes.
In young children, endotoxins quite quickly lead to irritation of the receptor apparatus of enterocytes, changes in enzymatic activity, secretion, absorption and, as a result, impaired gastrointestinal motility. Thus, impaired intestinal protective barrier increases the load on the enzyme systems of the liver and, under certain conditions, contributes to metabolic and structural changes in the organ. In pathological conditions, a vicious circle of dysmetabolic changes occurs, which contributes to the accumulation of intermediate products of impaired metabolism and endotoxins, which leads to the development of endogenous intoxication. In this regard, from the point of view of clinical physiology, methods of detoxification using sorption drugs are of particular relevance in the complex therapy of liver damage in children.
The clinical effectiveness of enterosorption in liver diseases is due to various mechanisms of action of enterosorbents. The main effect is realized by a direct detoxifying effect on toxic metabolites and toxins of the intestinal microflora, which, according to some reports, has negative changes in liver diseases [1]. An important mechanism of action of enterosorbents is the effect on the enzymatic saturation and concentration of biologically active substances in the gastrointestinal mucosa, which determine the manifestations of dyspepsia in diseases of the hepatobiliary system. In addition, sorbents have the property of increasing, due to concentration and osmotic gradients, the removal of endotoxins from the internal environment of the body into the intestinal cavity. This mechanism determines the role of enterosorbents in liver damage, regardless of their etiology.
Today, several groups of enterosorbents are defined: hydrocarbon, silicon-containing, natural organic based on dietary fiber, lignin, pectins, natural and synthetic resins, synthetic polymers [4]. One of the most widely used in pediatrics are silicon-containing sorbents, in particular Atoxil. A significant difference of the sorbent is the non-porous structure, the absence of which ensures a high rate of absorption processes, the maximum effect of which is manifested after 4 minutes.
Atoxil has protein-binding properties, which gives it the ability to adsorb pathogenic microorganisms from the gastrointestinal tract and remove toxic substances of various origins from the body, including allergenic microbial endotoxins. Atoxil is a domestic drug and meets the basic requirements for sorbents: non-toxic, does not injure the gastrointestinal mucosa, is easily evacuated from the gastrointestinal tract, has good sorption and organoleptic properties.
The aim of our work was to study the effectiveness of the use of the sorbent Atoxil in the complex therapy of children with liver damage associated with intestinal dysbiosis.
Research material and methods
We observed 34 children aged 1 to 3 years with liver damage associated with intestinal dysbiosis.
The main group consisted of 14 children: 9 children with infectious and cryptogenic hepatitis, 5 had damage caused by metabolic disorders (3 children with cystic fibrosis, 1 with glycogen storage disease, 1 with celiac disease).
The control group consisted of 20 patients with liver damage, comparable in age, who were treated in our department without including any sorbents in the therapy.
The examined children received standard complex treatment with antiviral agents, hepatoprotectors, probiotics, vitamins, and the children of the main group received the drug Atoxil. The drug was used at the rate of 150 mg/kg of body weight per day, administered 1 hour before or 2 hours after meals, three times a day.
Recommended doses of Atoxil: for children 1–2 years old, the daily dose is 2 g, 2–4 years old — 3 g, 4–7 years old — 4 g, 7–12 years old — 5–6 g, over 12 years old — 8 g. Other medications were taken 2 hours after taking the sorbent. The course of treatment was 14 days.
Research results and their discussion
Clinical symptoms in the examined children were characterized by specific clinical and laboratory manifestations: hepato- and splenomegaly, dyspeptic and hemorrhagic syndromes, increased transaminase levels. The main manifestation, according to the physical examination, was hepatomegaly (85.7% of children in the main group and 85.0% of children in the control group), which persisted steadily during the observation period, the degree of manifestations did not always correspond to the severity of the disease. With high activity of the process, liver enlargement was accompanied by changes in its consistency. Hepatomegaly was accompanied by an increase in the spleen in 35.7% of children in the main group and 30.0% of children in the control group. Hemorrhagic syndrome occurred during the active process (21.4% of children in the main group and 15.0% of the control group), was concomitant with severe hepatitis, and was characterized by bleeding from injection sites and the appearance of hemorrhages on the skin and mucous membranes.
Characteristic biochemical changes in the blood for patients with hepatitis of various etiologies were: prolonged hyperbilirubinemia, mainly due to conjugated bilirubin, persistent increase in liver cell enzymes (ALT, AST, LDH, GGT, etc.); increased globulin fractions, decreased albumin and blood clotting factors (prothrombin, fibrinogen, etc.). The activity of transaminases correlated with the severity of the course. The activity of the process was assessed by the concentration of transaminases. Minimal activity was characterized by an increase in transaminases to 1.5–2 norms, low - to 3–5 norms, moderate - to 9 norms, and high - above 10 norms. A normal level of transaminases in the absence of pathological changes in other biochemical indicators that characterize the functional state of the liver was regarded as an inactive process. Among the examined children, low-activity forms of the disease prevailed (57.1% of children in the main group and 60.0% of the control group). This course of hepatitis was accompanied by rather mild clinical symptoms. Moderate and high activity of the process was noted in 42.9% and 40.0% of the examined children, respectively.
Signs of cholestasis in the form of jaundice of the skin and mucous membranes, episodes of acholic stool were observed in 57.1% children of the main group and 60.0% children of the control group, although its classic manifestations in the form of persistent itching were not observed in the examined children. Dyspeptic syndrome, which was registered due to functional disorders of the gastrointestinal tract (appetite disorders, flatulence, bowel disorders), was detected in 92.0% children of the main group and 90.0% children of the control group. Intoxication disorders dominated the clinical picture of the examined children. Intoxication syndrome was observed in all patients and was characterized by pallor, lethargy, poor appetite, weight loss, muscle hypotension, hyporeflexia, and abdominal distension. Some children had low dynamics of body weight gain. In general, the clinical picture of the disease, with the exception of hepatomegaly, was characterized by a pronounced lability of clinical symptoms. The general condition of children in most cases was recorded as moderate and was observed in 64.21% of children in the main group and 70.01% of children in the control group.
The criteria for the effectiveness of treatment were the dynamics of the main clinical manifestations (intoxication and dyspeptic disorders) and laboratory indicators of microbiological examination of feces. According to the developed observation protocol, the presence and degree of manifestations of the main clinical symptoms were assessed on a point scale (2 - pronounced symptom, 1 - weakly pronounced, 0 - symptom absent) before the start of treatment, on the 7th and 14th days of observation. When analyzing the duration of objective manifestations of the disease, the general condition and irritability of the child were taken into account as manifestations of intoxication syndrome.
All examined patients had clinical manifestations of dysbacteriosis and were manifested by decreased appetite, flatulence, intestinal colic, and changes in the nature of defecation. Bacteriological examination of feces was carried out by the classical method; to assess the state of the intestinal microbiocenosis, the number of bacteria in feces was determined by inoculation of serial dilutions on differential diagnostic media (Methodological recommendations No. 10-13/3114/1U 1986). Dysbiosis was assessed according to the classification of I.B. Kuvaeva and K.S. Ladodo (1991) [2].
The first stage is the latent phase of dysbiosis. A decrease of 1–2 orders of magnitude in the number of bifidobacteria (BB), lactobacteria (LB), as well as full-fledged Escherichia coli to 80% of the total number. Other indicators correspond to the physiological norm (eubiosis). There are no clinical manifestations of dysbiosis in this phase.
The second stage is the starting phase. It is characterized by a pronounced deficiency of BB against the background of a normal or reduced amount of LB or a decrease in their acid-producing activity, an imbalance in the quantity and quality of E. coli, among which the proportion of lactose-negative or citrate-assimilating variants increases. The number of either plasmacoagulant staphylococci, or Proteus, or fungi of the genus Candida increases. Functional digestive disorders are expressed indistinctly - sporadic loose stools of a greenish color, with a shift in pH to the acidic side, sometimes delayed defecation.
The third stage is the phase of aerobic flora aggression. An increase in aggressive microorganisms: Staphylococcus aureus, Proteus, hemolytic enterococci; there is a replacement of full-fledged Escherichia with bacteria of the genus Klebsiella, Enterobacter, Citrobacter, etc. Functional intestinal disorders in the form of motility disorders, enzyme secretion and absorption.
The fourth stage is the phase of associative dysbiosis, characterized by a deep imbalance of the intestinal microbiocenosis with changes in the quantitative ratio of the main groups of microorganisms, changes in their biological properties, and the accumulation of toxic metabolites.
Table 1
Frequency of disturbances in the colonic microbial spectrum in children with liver damage

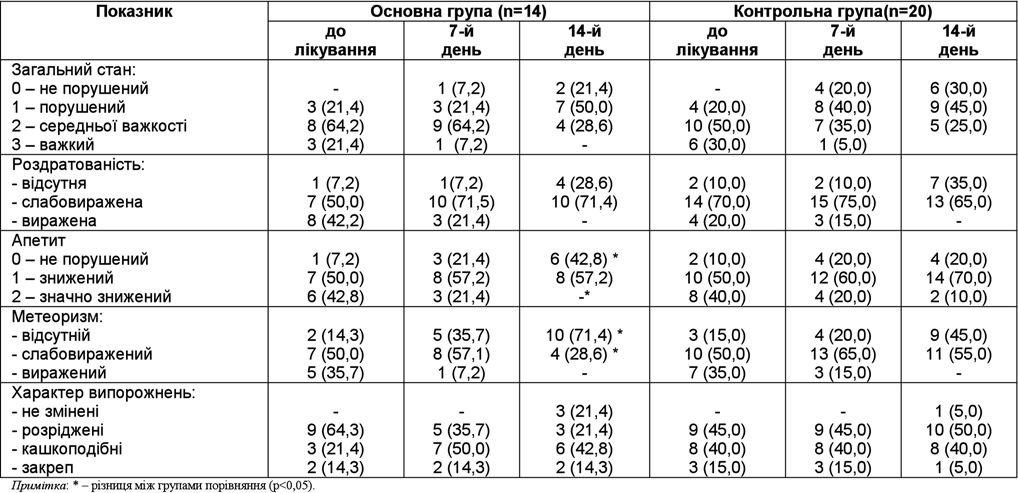
Table 2
Dynamics clinical symptoms in surveyed children in process treatment, abs/%
Vegetation of enteropathogenic serotypes of E. is characteristic. coli, salmonella, shigella and other pathogens of acute intestinal infections. Clostridium reproduction is possible.
Analysis of microbiological studies of feces revealed changes in patients of both groups (Table 1).
The characteristics of the microbial landscape in children with liver damage were manifested by a deficiency of bifidobacteria (<109 CFU/g) and lactobacteria (<107 CFU/g), an increase in the number and change in the species ratio of opportunistic bacteria. Thus, among children, a probable suppression of bifidobacteria (57.1% of children in the main group and 70.0% of children in the control group), lactobacteria (64.2% and 55.0%, respectively), Escherichia coli (57.1% and 30.0%, respectively); its enzymatic properties were changed in 42.8% and 50.0%, respectively. The quantitative decrease was accompanied by an increase in the specific weight of opportunistic flora: Klebsiella pn, S. aureus, enterococci. In children of both groups (21.4% of children of the main group and 15.0% of the control group), an association of several types of opportunistic microorganisms in various combinations was established. In children of both groups, comparable changes in the composition of the intestinal microflora were found, the degree of dysbacteriosis did not have significant differences.
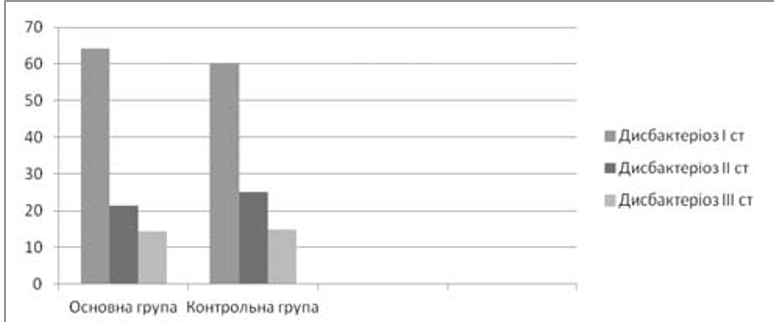
Rice. 1. Distribution of sick children by degree of dysbacteriosis at the beginning of observation, %

Rice. 2. Distribution of sick children by degree of dysbacteriosis on the 14th day of observation, %
Thus, in the main group, dysbacteriosis of I and II degrees was recorded in 9 (64.2%) and 3 (21.4%) children, dysbiosis of III degree was observed in 2 (14.3%) cases. In the control group, dysbacteriosis of I degree was detected in 60.0%, II — in 25.0%, III — in 15.0% cases (Fig. 1).
Analysis of the dynamics of clinical symptoms showed the effectiveness of treatment in both groups. During the analysis of the duration of objective manifestations (intoxication and dyspeptic), changes were found between the comparison groups in terms of appetite and bloating. The dynamics of clinical symptoms of the course of the diseases are presented in Table 2.
The rate of normalization of dyspeptic manifestations in the form of flatulence and appetite disturbance on the 7th day of treatment was the same in both groups of patients, and on the 14th day a significant increase was noted in children in the main group (42.8% of children in the main group versus 20.0% of children in the control group); the disappearance of flatulence occurred in 71.4% of patients in the main group and only in 45.0% of children in the control group.
There was also an improvement in the characteristics of bowel movements in the main group: on the 14th day, improvement was noted in 42.81% of children in the main group, and in the control group - only in 15.01% of children. It should be noted that in 2 children who had bowel movements with a tendency to constipation, the nature of the stool did not change against the background of the use of Atoxil.
Children in the main group who took Atoxil for 2 weeks, as evidenced by the conducted clinical analysis, had significant changes in clinical signs of dysbacteriosis (bloating, nature of stools). Microbiological control of stools showed that in 42.81% of the examined patients after treatment with Atoxil, the intestinal microbiocenosis normalized, while in the control group - only in 15.01% of cases (p<0.05) (Fig. 2).
As can be seen from the data presented, among children who took Atoxil, 42.8% had complete normalization of microflora, and among children in whom dysbiotic changes remained, their severity significantly decreased: most of them (75%) had dysbiotic changes of the 1st degree, and no patients with dysbacteriosis of the 3rd degree were noted.
In the group of children who did not use the sorbent, the control indicators were significantly lower: normalization of microflora was observed only in 15.0%, and among children with dysbiotic changes, dysbacteriosis of the I degree was observed in 52.9%, in 41.2% — in the II degree, and in 1 child dysbiotic changes of the III degree remained.
Quantitative assessment of microbial flora in children of both groups allowed to establish a significant decrease in intestinal contamination with opportunistic flora: in the main group its increase was registered only in 3 children. In the comparison group no significant changes were detected.
Conclusions
Comparative analysis of the effectiveness of treatment of children with liver damage indicates a significantly faster dynamics of elimination of intestinal dysbiosis when using Atoxil. The results of the studies indicate the feasibility of its use in the complex treatment of sick children with liver damage of any etiology associated with intestinal dysbiosis. The drug is well tolerated, no cases of intolerance or side effects were noted during use.
LITERATURE
- Denisova M.F. The use of probiotic lactiv-ratiofarm in the complex treatment of chronic viral hepatitis in children / M.F. Denisova, N.N. Muzyka, T.A. Lysyanaya // Sovr. pediatrics — No. 6 (28).
- Kuvaeva I. B. Microecological and immune disorders in children / I. B. Kuvaeva, K. S. Ladodo. — M.,
- Kucherenko N. P. Microbiocenosis of the large intestine in patients with viral hepatitis / N. P. Kucherenko, A. I. Bobrovytska, I. O. Vereshchagin // Materials of the scientific-practical conference and plenum of the Association of Infectious Diseases of Ukraine. — Ternopil, 2004. — P. 115—116
- Enterosorption: the state of the question and prospects for the future / Nikolaev V. G., Mikhalovsky S. V., Nikolaeva V. V. [and others] // Visn. problems of biology and medicine. — Vol. 4. — P. 7-17.