UDC: 616.36 – 002.14-022:578.891-085.03
APPLICATION OF ENTEROSORBENT "ATOXYL" IN THE TREATMENT OF PATIENTS WITH ACUTE HEPATITIS A AND B
O.A. HOLUBOVSKAYA, N. C. KORCHINSKY
National Medical University named after A.A. Bogomolets, Department of Infectious Diseases
Key words:
hepatitis A, B, treatment, enterosorbents, enterosorption, Atoxyl
The relevance of improving the treatment of patients with hepatitis A and B is due to the preservation of a sufficiently wide spread of these infections both in the world and in Ukraine, the absence of etiotropic treatment for hepatitis A (HA) and agreed recommendations for the use of antiviral drugs in acute hepatitis. Despite the decrease in morbidity, there is a large economic loss from hepatitis A, which in 2006 amounted to more than 1 billion rubles in the Russian Federation, and in 2009 - about 834 million [10, 15]. Previously, GA was observed mainly in children and belonged to the group of so-called "childhood" diseases. In children, mainly mild forms of the disease are observed, without jaundice in 75-80% of all cases of the disease. But recently, in Ukraine, there has been a significant increase in the incidence of GA among the adult population, with a predominance of more severe forms accompanied by jaundice, a significant duration of the disease, and a generally more severe course. The incidence of GA in Ukraine in recent years was 24.8–26.3 cases per 100,000 population, which is significantly higher than in most European countries [9,10].
The problem of diagnosis and treatment of GV is even more important. Thus, about a third of the world's population has serological signs of past or current infection caused by HBV. According to WHO experts, 300 to 400 million people are infected with this pathogen. According to various reports, 15 to 40% of them have chronic hepatitis B (HCV) progressing to liver cirrhosis (CP) and hepatocellular carcinoma (HCC), which at any stage can be complicated by liver failure and lead to fatal consequences [7, 16, 19, 21]. Despite the availability, effectiveness and safety of specific vaccines, HBV remains the 1st place in the world among all causes of death of patients with liver pathology. From liver diseases caused by HBV, 1 to 2 million patients die annually in the world, including 0.5 to 1 million patients from HCC alone (5th place among lethality from malignant tumors). Every year, the terminal stages of HBV infection are the cause of 5 - 10% of all liver transplants in the world. Among all causes of death, the consequences of CHB occupy the 10th place in the world [16, 18, 19, 21]. Special long-term studies show that 5 years after the diagnosis of CHB, the total frequency of CP development ranges from 8 to 20%, and the 5-year cumulative frequency of decompensation of liver functions is about 20% with a total 5-year survival probability of 80 – 83% of patients with compensated CP. The annual frequency of occurrence of HCC in patients with CHB and CP is 2-5% [18, 20, 21].
At least 1 million people are recognized as carriers of HBV in Ukraine. Every year, 188,000 patients with CHD and CP are officially registered in our country, of which 6,000 die annually. Markers of HBV infection: HBsAg and anti HBcor in Ukraine are found in 1.4% and 13.9%, respectively, in blood donors, in medical workers – in 5.4% and 26.8%, in people who use intravenous drugs – in 15.05% and 50.55% [7, 9].
Patients with mild and moderate forms of acute hepatitis A and B do not need not only etiotropic, but also drug therapy in general [17, 18]. Nevertheless, the search for drugs that can have a positive effect on the course of the disease, reduce the duration and severity of intoxication and jaundice syndromes, while not causing serious side effects and not worsening the outcome of the disease [7, 8, 11], continues.
First of all, enterosorbents belong to similar drugs.
Enterosorption as one of the methods of detoxification therapy has become quite widespread in clinical practice. This method is characterized by its simplicity, safety and economy, therefore it is successfully used in the treatment of various liver diseases, including VL [7, 8, 11, 12, 13].
Important mechanisms of action of enterosorbents include:
- binding of toxic substances entering the gastrointestinal tract from the outside;
- binding of toxins that diffuse into the intestinal lumen from the blood;
- binding of toxic substances released with digestive juices;
- absorption of toxic metabolites formed in the gastrointestinal tract;
- sorption modification of the diet due to the selective absorption of some amino acids and free bile acids;
- fixation and transfer of physiologically active substances (enzymes, bile acids, etc.);
- changing the volume of the part of food that is not digested;
- catalytic action;
- enveloping and cytoprotective action;
- structuring of intestinal contents;
- formation of aggregates and flocculates containing microbes and viruses;
- direct bactericidal action;
- complex formation and chelation;
- modification of the chemical composition of intestinal contents, which becomes unfavorable for the reproduction of pathogenic microflora [8, 12, 14].
As a result of the implementation of the specified mechanisms, enterosorbents reduce the toxic load on the liver and kidneys. Enterosorbents, not being absorbed into the blood, nevertheless have a significant systemic effect on the body, eliminating disorders of lipid metabolism, suppressing the systemic inflammatory reaction, contributing to the compensation of individual parts of the immune system and improving the function of internal organs, which is very important in patients with acute viral hepatitis [8, 11, 12, 14].
As a result of a violation of metabolic processes in patients with acute hypertension, the syndrome of metabolic intoxication develops, caused by the accumulation in the blood of molecules of medium weight, which have a toxic effect on the cells of the liver, kidneys, and neurons of the brain. With a severe course of VH, ammonia and aromatic compounds accumulate in the intestines, and then in the blood, causing the development of toxic encephalopathy and hepatic coma [7, 12].
In Ukraine today, there is a fairly large selection of enterosorbents, which have different chemical structures, physico-chemical and organoleptic properties, and differ in various clinical effects. The area of the active surface is the basis for determining the effectiveness of a particular sorbent. It is inversely proportional to the size of the particles - the smaller the size of the particles, the greater the total area of their active surface. Therefore, its capacity depends on the dosage of this or that enterosorbent, which provides the optimal therapeutic effect [8, 12].
Table 1
Comparison of enterosorbents, usually used in practical health care of Ukraine (V.N. Nagornaya, 2005)
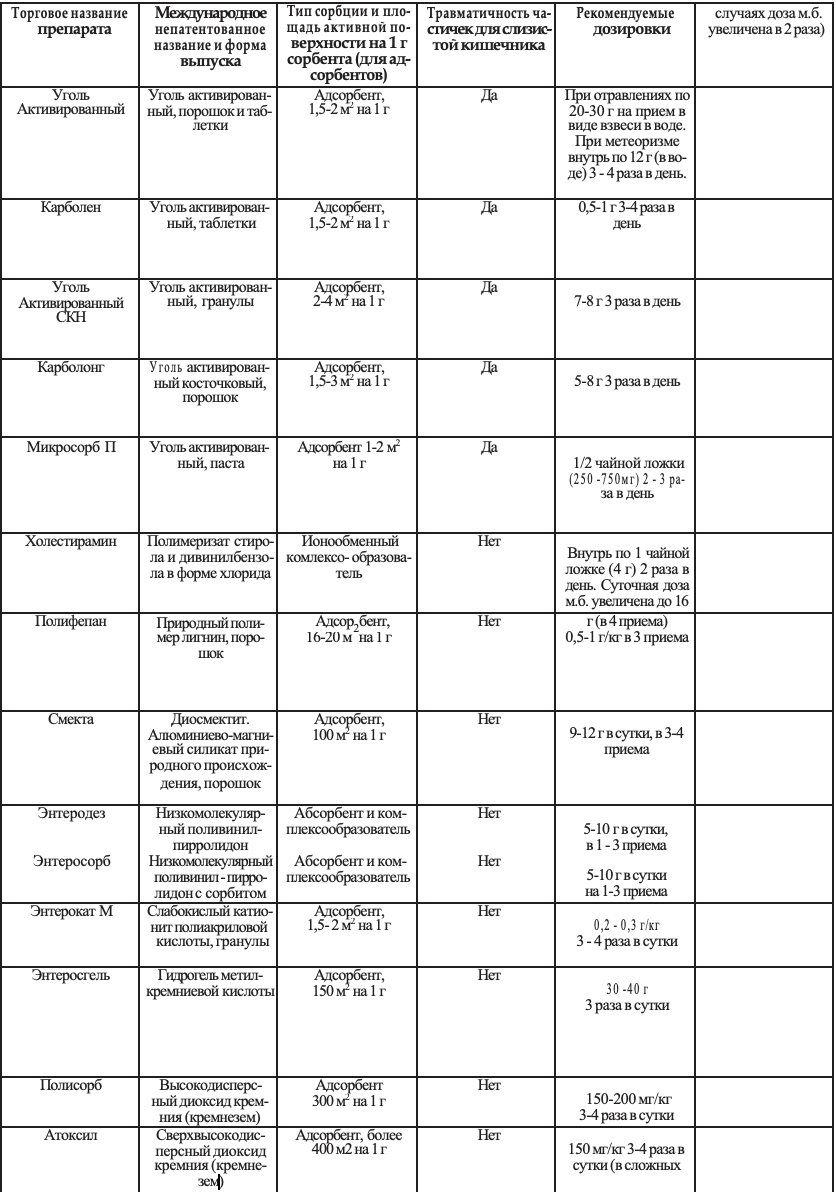
Sorbents based on activated carbon have a small area of active absorption surface per 1 gram of the active substance. Therefore, with significant endogenous intoxication, it is necessary to take 20-30 grams of them per day (80-120 tablets of activated carbon), which causes a much lower attractiveness of carbon sorbents compared to modern sorbents, especially those based on silicon dioxide [8].
A comparison of enterosorbents commonly used in practical healthcare in Ukraine is given in Table 1. Due to the high sorption activity of silicon dioxide preparations (Table 1), endogenous and exogenous toxic substances are more intensively absorbed and removed from the gastrointestinal tract, in particular, the products of the life of pathogenic microorganisms. The drugs are not absorbed from the alimentary canal, while providing powerful systemic detoxification.
It should also be noted the selectivity of adsorption of preparations based on silicon dioxide, which determines their advantages compared to other preparations [8, 12, 13]. The corresponding materials are presented in Table 2. Thanks to the properties listed above, preparations based on silicon dioxide had a positive effect in:
- diarrhea of infectious and non-infectious origin;
- colitis;
- acute and chronic viral hepatitis;
- botulism;
- intestinal toxicosis;
- chronic obstructive lung diseases;
- bronchial asthma;
- chronic renal failure;
- eczema, psoriasis;
- atopic dermatitis;
- late gestosis of pregnant women;
- in surgical practice;
- in toxicology;
- in oncology [1, 3, 4, 5, 6, 7, 8, 11, 12, 13, 14].
Previously conducted clinical studies [7,8,11] are mainly concerned with hydrogel of methylsilicic acid, while there are few studies of the effectiveness of other preparations based on silicon dioxide. At the same time, the most effective in the fight against intoxication in patients with various liver pathologies are sorbents prepared precisely on the basis of silicon dioxide, in particular Atoxyl, which is just beginning to be introduced into hepatological and infectious practice [4,5,7,11,12].
The preparation "ATOXIL" (silicon dioxide), which is produced by "Orisil Pharm" LLC, is silicon dioxide, is a light amorphous powder of white color, tasteless and odorless, in bottles with a capacity of 250 ml. 1 bottle contains 10.0 gr. highly dispersed silicon dioxide powder. The area of its active sorption equals more than 400 m² per 1 g of dry substance, which is one of the highest indicators among similar preparations (Table 1). ATOXIL is an enterosorbent with pronounced sorption properties, exhibits detoxification, and when applied topically it has antimicrobial and wound-healing effects [3,5,11,14]. The drug adsorbs from the digestive tract and removes from the body endogenous and exogenous toxic substances of various origins, has high adsorption activity against microorganisms and proteins, including microbial toxins. At the same time, the desorption of bound proteins and toxins worsens both through the wound and through the intestinal walls. ATOXIL promotes transport from the internal environment of the body (blood, lymph) to the digestive tract due to concentration and somatic gradients of various toxic products, including medium molecules, oligopeptides, amines and other substances with subsequent removal from the body. At the same time, it is practically not absorbed from the intestines and wounds [3,8,13,14]. Atoxyl is contraindicated in patients with exacerbation of peptic ulcer disease of the duodenum and stomach, erosions and ulcers of the mucous membrane of the large and small intestine, with intestinal obstruction, with increased sensitivity to silicon dioxide. Atoxyl is not prescribed to children under one year of age and pregnant women [5,14].
As shown by clinical and laboratory studies, the drug ATOXIL is effective in the complex treatment of burns and the prevention of infectious complications in burned patients. It was satisfactorily tolerated by patients when used orally and topically, without causing side effects. Complex detoxification therapy using the drug ATOXIL led to a decrease in the toxic properties of blood serum, provided a significant decrease in the toxic effect on neutrophil granulocytes of peripheral blood, as indicated by the integral indices of intoxication [14]. Experimental confirmation of the positive effect of Atoxyl on periapical tissues in the treatment of periodontitis was obtained [3]. The combination of Atoxyl and quercetin improved the results of the treatment of patients with peptic ulcer of the duodenum against the background of hypertension, eliminating at the same time violations of metabolic indicators [1,2]. Atoxyl increased the effectiveness of complex therapy of ascariasis in children [4]. The effectiveness and safety of Atoxyl treatment of acute intestinal infections in children has been confirmed [5]. At the same time, we did not find information about the use of this drug in patients with acute or chronic viral hepatitis. This determined our choice in the study of the clinical effectiveness of this enterosorbent in patients with acute VH.
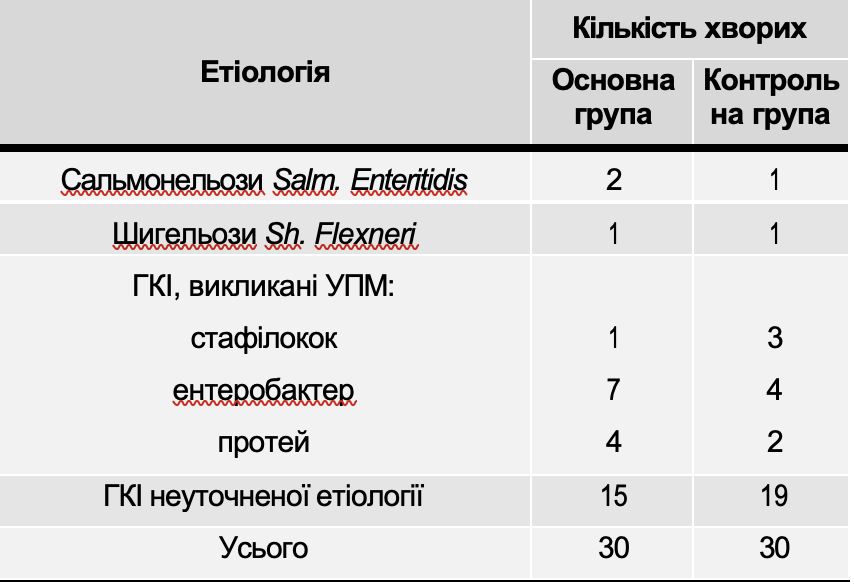
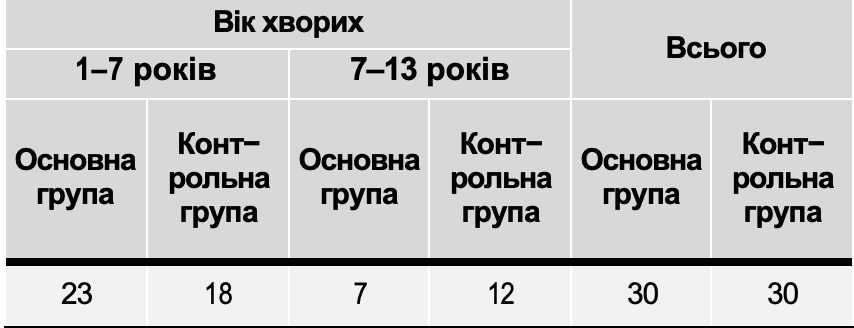
According to the set tasks, in the clinic of infectious diseases of NMU during 2010-2012. examined and observed 71 patients with HA and acute HF with a mild course of the disease aged from 18 to 62 years (average age of patients – 34.6±8.2 years). Patients aged 18 to 35 years predominated (52 people, 73%). There were 32 men, 39 women. A mild form of jaundice was present in 19 (26.8%) patients, and a moderate form in 52 (73.2%) patients. To study the therapeutic effect of the enterosorbent Atoxyl, all patients were divided into two groups comparable in age, gender, and nature of concomitant diseases by the method of randomization. Since the effect of the drug on the duration of HBs-antigenemia and viremia was not studied, it was considered possible to combine in one group patients with HA and acute HB, the distribution of which in the groups also did not differ: 7 patients with HA in each group (Fig. 1).
Patients of the 1st group (36 people) received Atoxyl treatment. Patients of the 2nd group (35 people) received only basic therapy. The general characteristics of groups of patients are presented in Fig. 1.
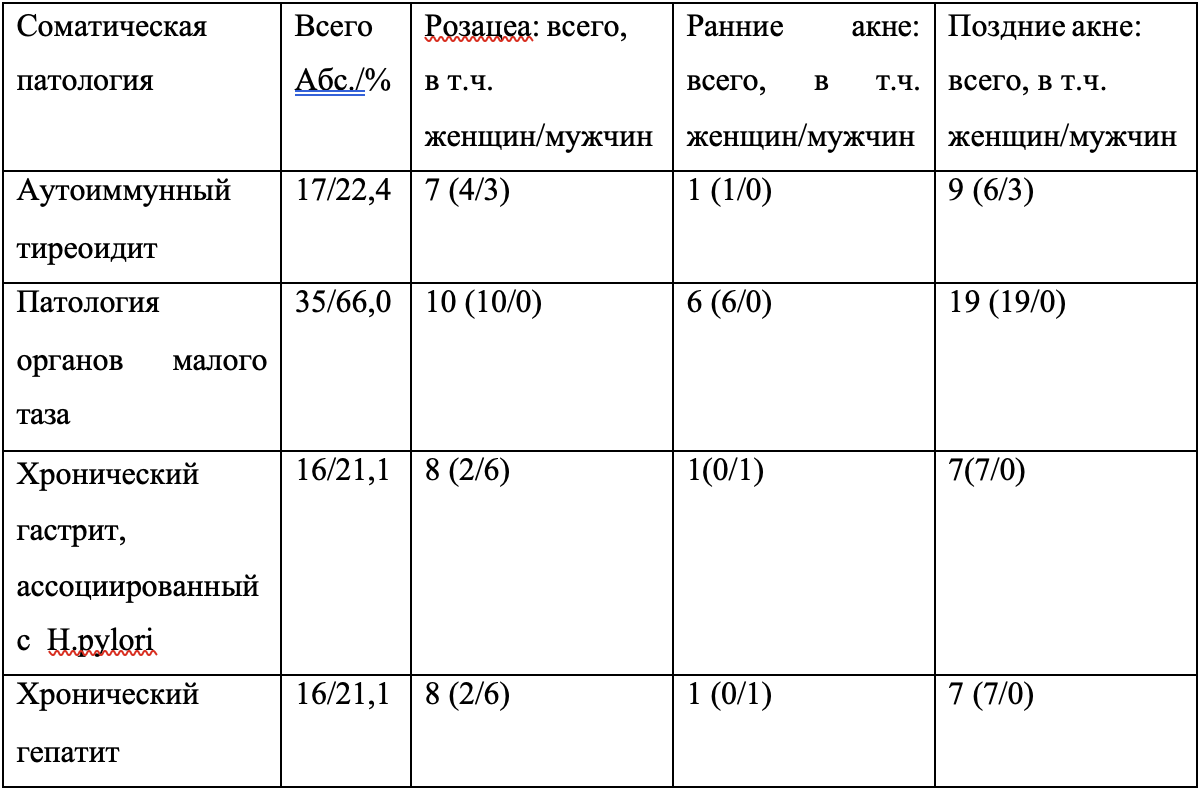
As can be seen from the data shown in Fig. 1, according to the main parameters - gender, age, severity of hypertension and its etiology, the groups of patients were comparable. The most common concomitant disease was chronic pancreatitis in 43 (60.6%), exacerbation of chronic gastroduodenitis in 21 (29.6%), cholecystitis in 19 (26.8%), fatty liver disease in the form of nonalcoholic and alcoholic steatohepatitis in 16 (22.5%), chronic bronchitis in 9 (14.6%). On Fig. 2 presents the characteristics of groups of patients depending on the nature of the accompanying pathology, which most often occurred against the background of VH.
As can be seen from the materials shown in Fig. 2, there were also no significant differences in the nature of accompanying pathology between the 1st and 2nd groups.
Patients with severe somatic concomitant pathology (decompensated diabetes mellitus, severe atherosclerosis, severe arterial hypertension, etc.) were not included in the study, as they required constant intake of a significant amount of medication. HIV and HCV infection were ruled out in all patients.
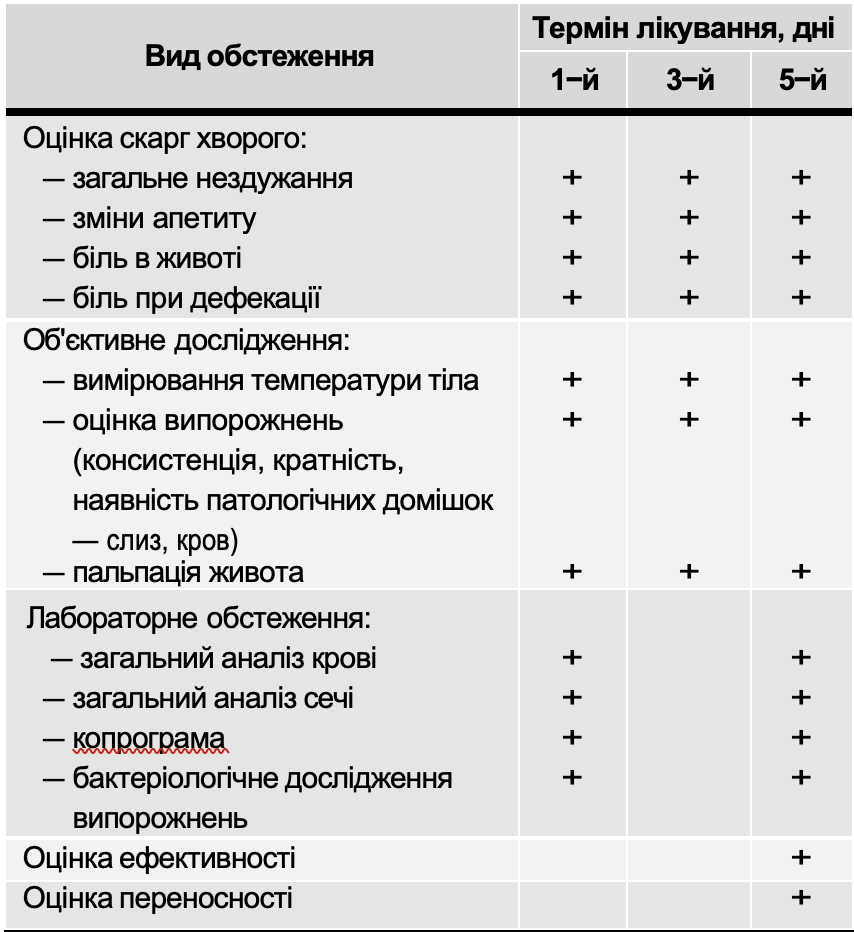
In all patients, indicators of general blood analysis, the content of glucose, total protein, total bilirubin and its fractions, urea, creatinine, activity of ALT and AST in the blood were studied dynamically with the help of generally accepted methods using standard reagents and the Humalaser biochemical analyzer. An ultrasound examination of the liver, gallbladder, pancreas, spleen, and kidneys was performed using a gray scale on an expert-class Voluson 730 SSD device. With the help of immunoenzymatic analysis (ELISA), the diagnosis of HA was specifically confirmed in 14 patients by the presence of AntiHAV Ig M in the blood, acute HBV - in 57 patients by the presence of HBsAg and anti HBcor Ig M in the blood. In doubtful cases (differentiation from chronic HBV), anti HBcor IgG, HBeAg, anti HBe Ig G were additionally quantified (ELISA).
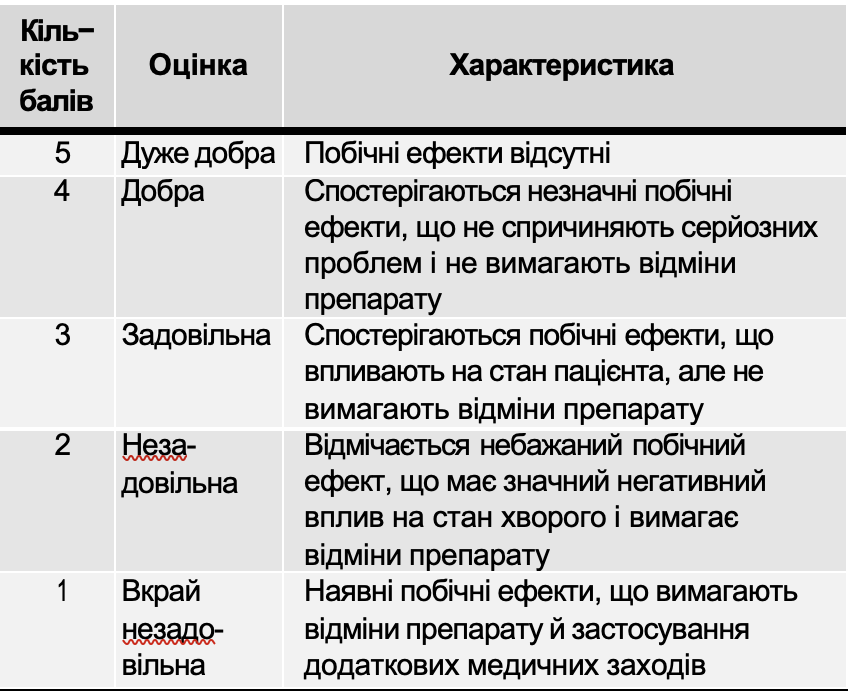
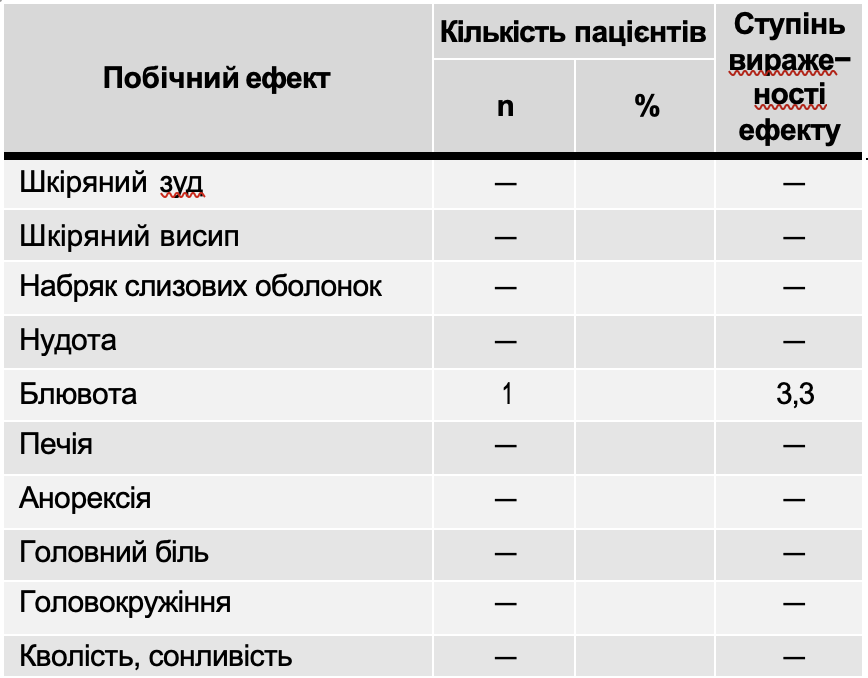
36 people of the first group on the background of generally recognized basic therapy (bed rest, table No. 5a, abundant drinking) from the moment of hospitalization in the clinic (on average, from 4.3±2.1 days of the jaundice period) received Atoxyl at the rate of 0.2 g per kg of body weight per day (on average 12 g) orally in 3 doses 2–1.5 hours before meals for 2 weeks. 35 people of the second group received only basic therapy during the same period of the disease. None of the patients had any serious side effects of Atoxyl that would require discontinuation of the drug. In one patient with concomitant exacerbation of chronic gastroduodenitis, a short-term increase in nausea was noted, in 3 patients - increased constipation, which required the prescription of Lactulose.
Table 2
Selectivity of adsorption of preparations based on silicon dioxide (according to A.A. Chuyko, 2003)
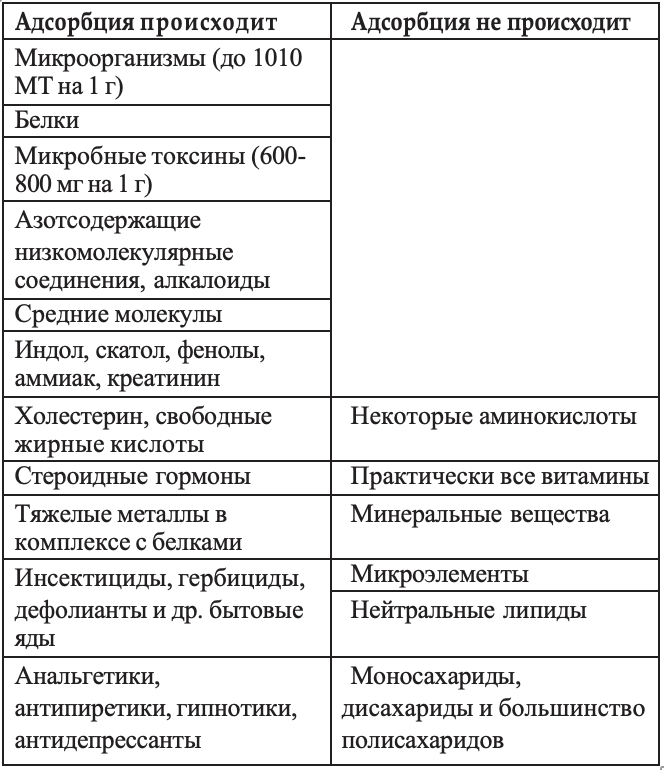
Figure 1. General characteristics of groups of patients
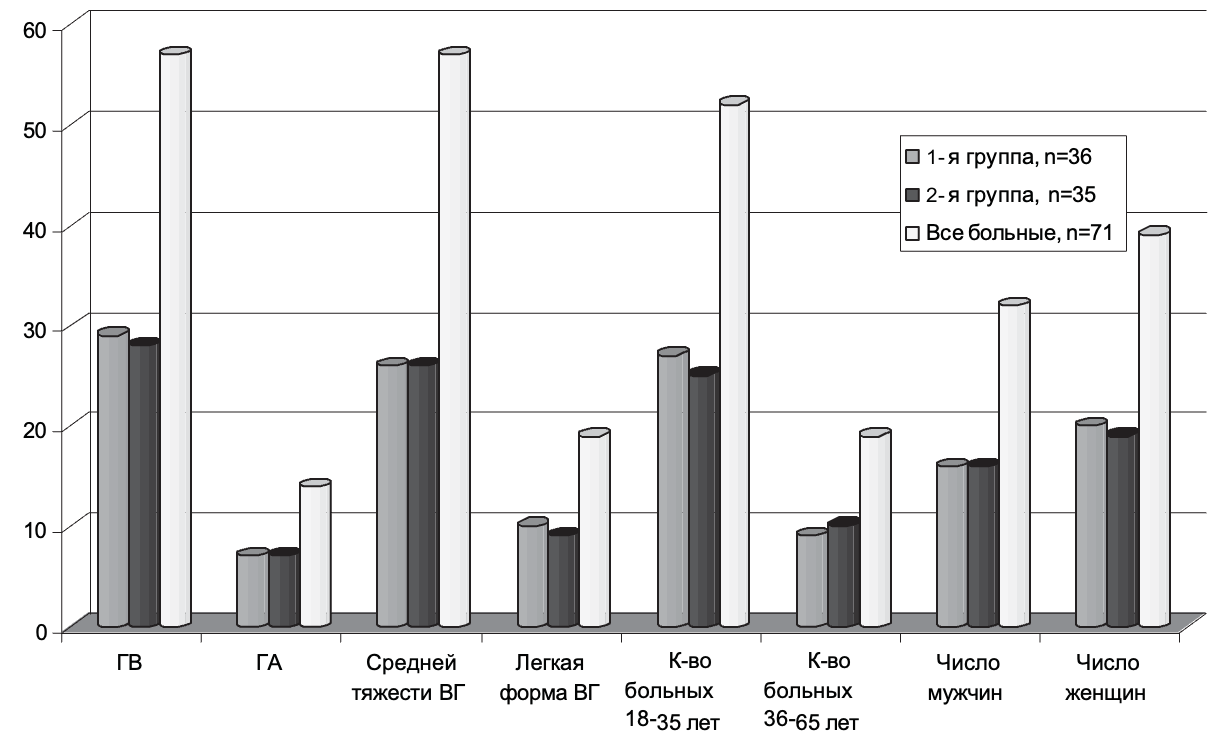
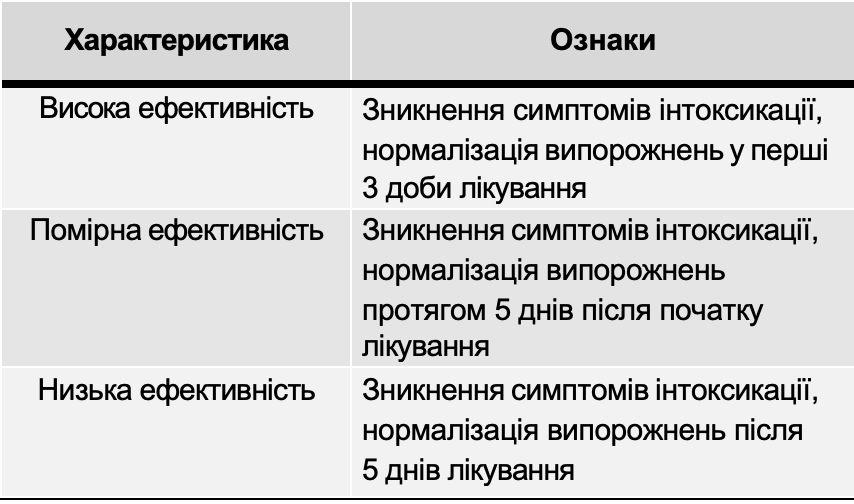
Table 3
Comparison duration clinical symptoms jaundiced period sharp VG in patients receiving Atoxyl and treated without it

Fig. 2. Characteristics of groups of patients depending on accompanying pathology.
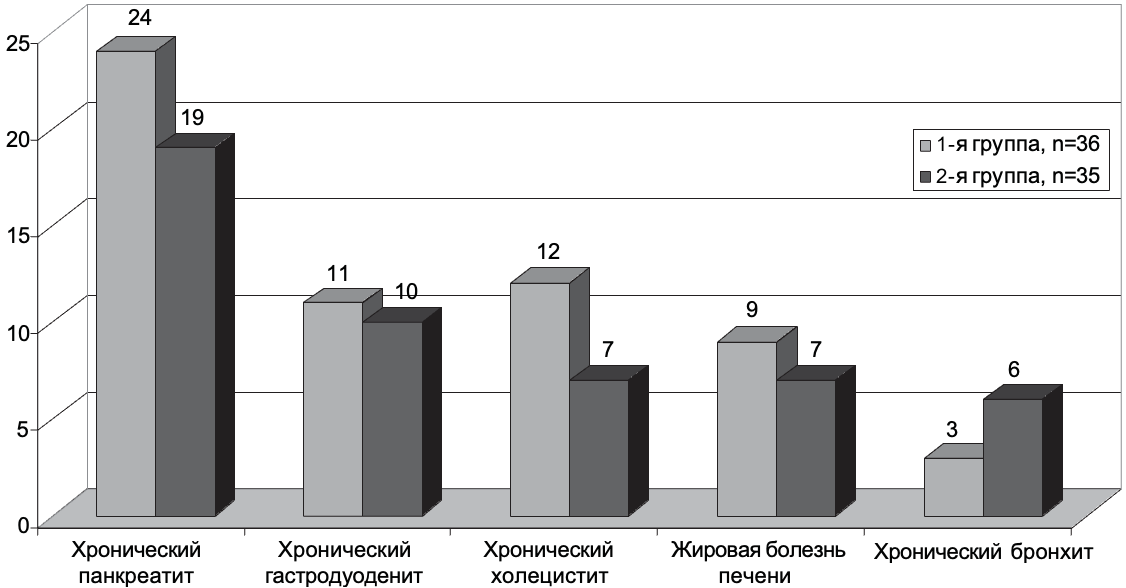
Table 4
Comparison of the average values of basic biochemical parameters of blood in patients of both groups before treatment with Atoxyl
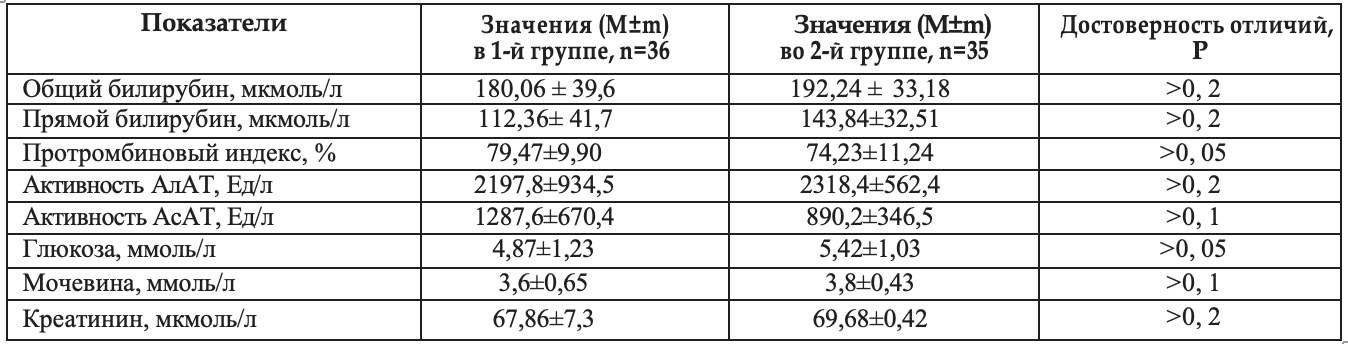
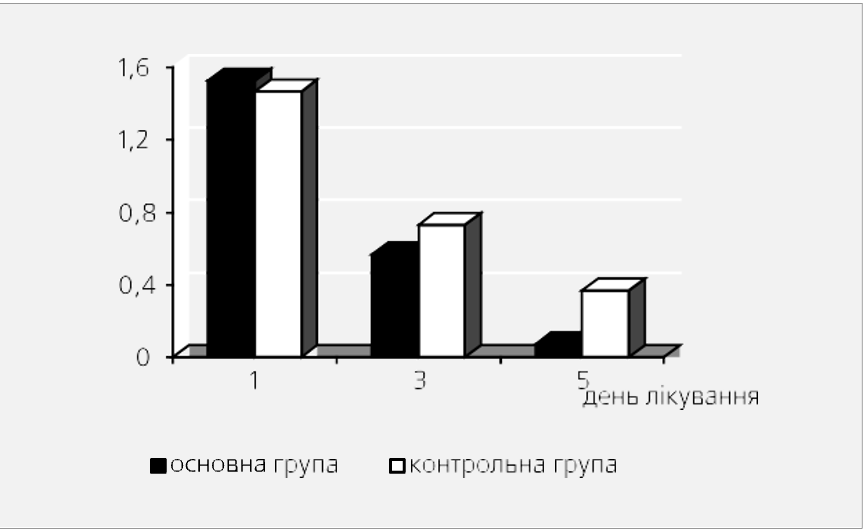
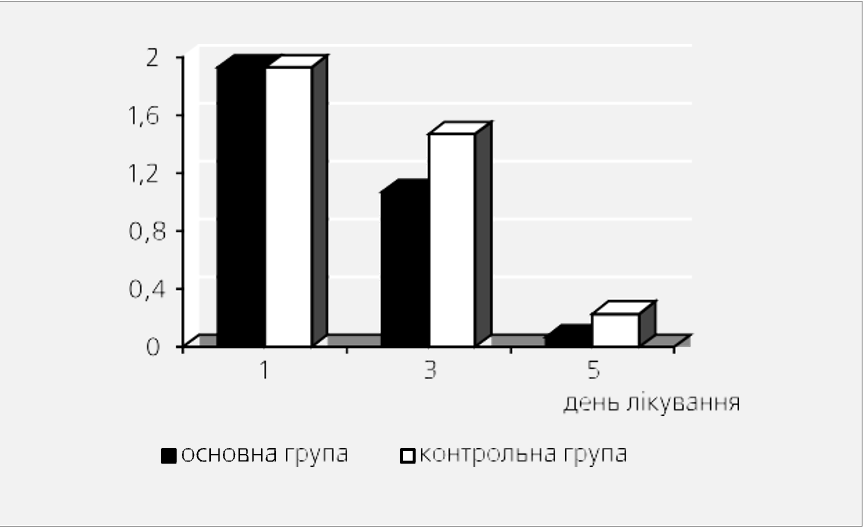
Fig. 3. Comparison of the average indicators of the duration of clinical symptoms during the treatment of patients with Atoxyl (n=36) and without it (n=35)
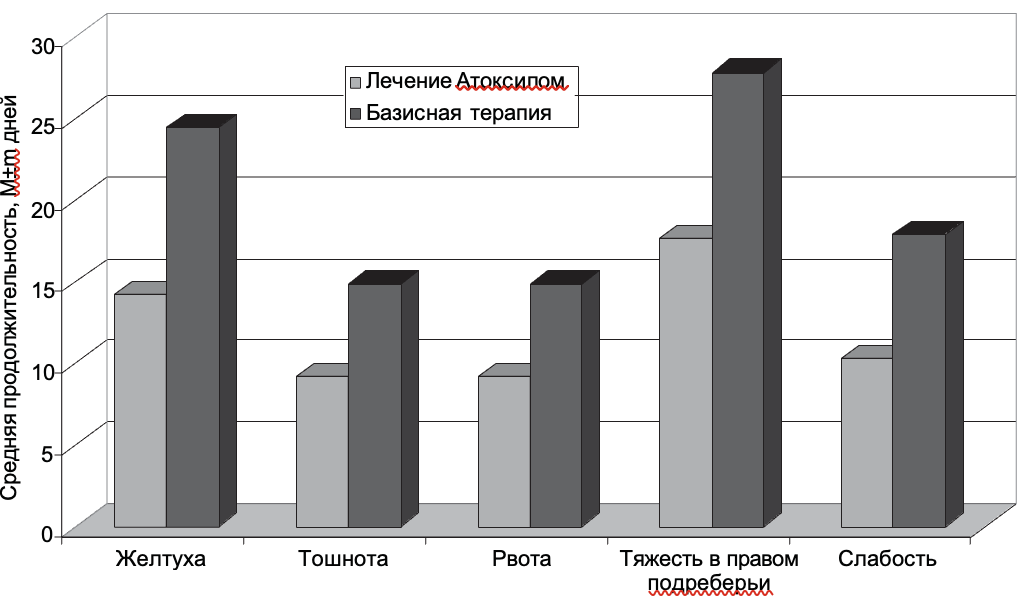
Table 5
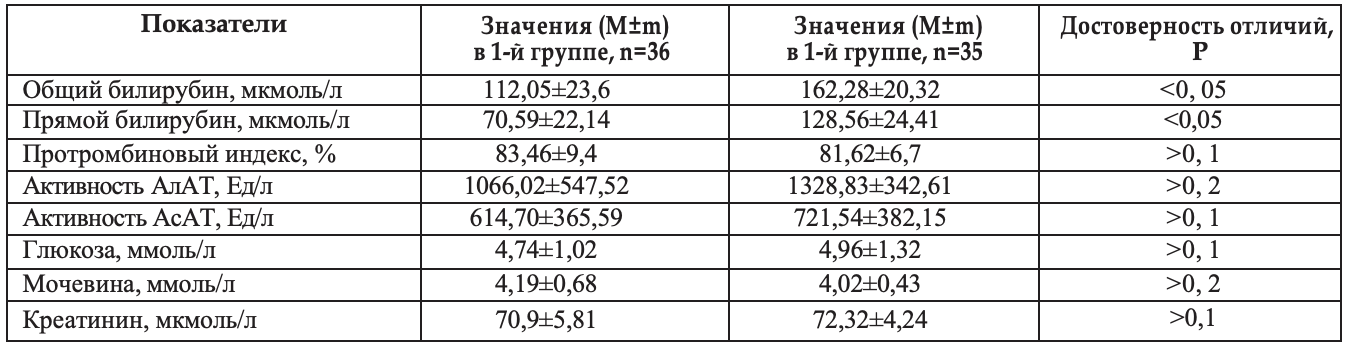
Comparison of the average values of basic biochemical parameters of blood in patients of both groups after treatment with Atoxyl
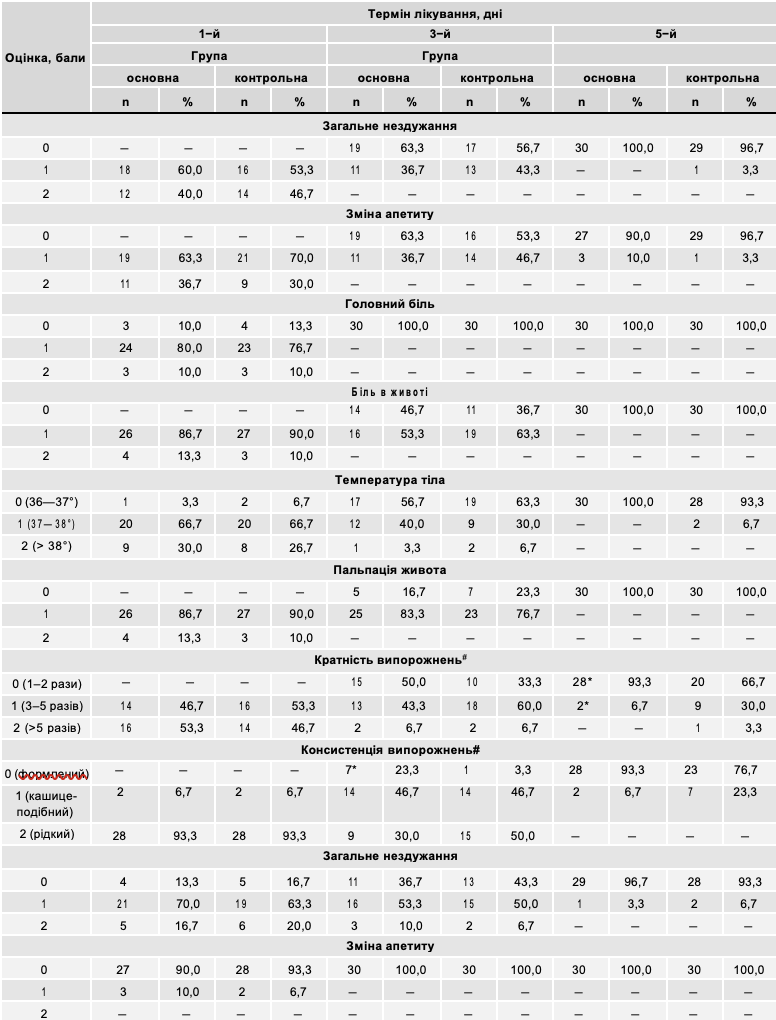
The duration of symptoms of the disease was analyzed in both groups. Corresponding data are presented in Table 3. As evidenced by the data presented in Table 3, treatment with Atoxyl significantly (Р<0.05) reduced the duration of jaundice, heaviness in the right hypochondrium, nausea, vomiting, and general weakness, thereby confirming its pronounced detoxification effect. Corresponding data are shown in Fig. 3.
As evidenced by the data shown in Fig. 3, treatment with Atoxyl causes significantly (Р<0.05) faster reversal of symptoms of the disease, such as jaundice, weakness, heaviness in the right hypochondrium, nausea, vomiting compared to the average duration of similar symptoms in patients of the comparison group.
The main analyzed biochemical blood parameters before the onset of the disease in both groups were not significantly different (Table 4), so the analysis of parameters was carried out by us after 2 weeks of treatment with Atoxyl.
As evidenced by the materials presented in Table 4, there were no significant differences in any of the compared average indicators of biochemical blood parameters. Table 5 presents the results of a comparison of the average values of the main biochemical parameters of the blood after treatment with Atoxyl.
As evidenced by the materials presented in Table 5, after treatment with Atoxyl, the average indicators of total bilirubin in the blood and its direct fraction decreased significantly more compared to those in patients who did not receive enterosorbents (Р<0.05 and <0.05, respectively). There were no significant differences in the average activity indicators of ALT, AST, PTI, blood glucose, creatinine, and blood urea in patients treated with Atoxyl compared to those in the comparison group.
Thus, treatment with Atoxyl at a dose of 12 g/day orally for 2 weeks in patients with non-severe acute hepatitis A and B reliably reduces the duration of dyspeptic and intoxication syndromes, the jaundice period, reduces the level of total and direct bilirubin compared to the same indicators in patients who received only basic therapy during the same period of the disease. The drug is well tolerated, does not cause negative emotions when taking it, is relatively inexpensive, convenient to use, does not cause serious side effects, which makes it possible to recommend it for wider use in the treatment of acute viral hepatitis.
LIST USED LITERATURE
- Belokobylskaya D.V. Changes in the content of leukotrienes and activity of lipoperoxidation under the influence of the combination of atoxyl and quercetin in the dynamics of treatment of patients with peptic ulcer of the duodenum in combination with hypertension / D.V. Belokobylskaya// Ukrainian medical almanac. – Volume 13, No. 4. - pp. 30-32.
- Burmak Yu.G. Changes in some metabolic parameters in the dynamics of treatment of patients with peptic ulcer of the duodenum in combination with hypertension / Yu.G. Burmak, D.V. Belokobylskaya //Tavricheskyi mediko-biologicheskiy vestnik. – 2010. – volume 13, number 1 (49). - P. 23 - 25.
- Dorofeeva N.G. Experimental confirmation of the influence of sorbents on periapical tissues in the treatment of periodontitis [Text] / N.G. Dorofeeva, T.A. Chalaya, M. Erokhina, A. Obydin // Ukrainian medical almanac. – 2008. – Volume 11, No. 5. - P. 61-62.
- Korneva V.V. Evaluation of the effectiveness of the enterosorbent Atoxyl in the complex treatment of ascariasis in children / V.V. Korneva, L.V. Kurylo, V.G. Kozachuk, E.A. Boyarskaya, M.A. Kapychyna //Sovremennaya Pediatriya. - #3(37). - P.66-68.
- Kramarev S.O. Study of the effectiveness and safety of the enterosorbent Atoxil in acute intestinal infections in children / S.O. Kramarev, O.A. Dmitrieva // Modern Pediatrics. – – No. 3. – P. 93-97.
- Kuznetsov S.V. Efficacy of enterosorbent White coal in complex therapy of helminth infections in children / S.V. Kuznetsov // Health of the child. – – №4. - p. 30-33.
- Treatment of patients with cirrhosis of the liver of predominantly viral etiology, complicated by ascites / Zh.I. Vozianova, O.A. Golubovska, M.Ch. Korchinsky //The Art of Treatment, 2005. – No. 5(21). – P. 22 – 27.
- Medicinal chemistry and clinical application of silicon dioxide/ Ed. Acad. National Academy of Sciences of Ukraine A.A. Chuyko. - Kyiv: Scientific Thought. – – 416 p.
- Ministry of Health of Ukraine //ORDER No. 296 dated 05/19/2011 “On Amendments to the Order of the Ministry of Health of Ukraine dated 02/03/2006 No. 48”
- Mykhailov M.I., Shahgildyan I.V., Onishchenko H.G. Enteral viral hepatitis (etiology, epidemiology, diagnostics, prevention) - Moscow: VUNMC, 2007 - 352 p.
- Moroz L.V., Paliy I.G. Use of the drug Enterosgel in the complex therapy of patients with acute viral hepatitis with concomitant intestinal dysbacteriosis / L.V. Moroz, I.G. Paliy // Medical and biological aspects of the use of the enterosorbent “Enterosgel” for the treatment of various diseases: Collection of selected scientific articles. –Kyiv: “Bogdana”, 2010. -P.83-88.
- Nagornaya N.V. The use of enterosorption in the treatment of atopic dermatitis / N.V. Nagornaya, E.V. Bordyugova, A.V. Dubovaya //Sovremennaya pediatriya. – 2005. – No. 4(9). - P.67 - 70.
- Paley I.H. A modern view of the problem of enterosorption: the choice of the optimal drug / I.G. Paly, I.G. Reznychenko // News of medicine and pharmacy. – No. 11 (217). - P. 15-17.
- The use of the drug "Atoxyl" in the complex treatment of burns / E.Ya. Fistal, I.I. Speransky, V.V. Arefiev, E.G. Tymoshenko, M.V. Lobacheva, E.A. Pisarenko // Combustiology. – No. 27.- P. 24-28.
- Shahgildyan I.V. Evaluation of the results of hepatitis A vaccine prevention in certain regions of the Russian Federation. Is routine vaccination of children against hepatitis A necessary today [Text]/ I.V. Shahgildyan, M.I. Mykhaylov, O.N. Ershova, P.A. Khukhlovych, V.A. Khasanova, I.N. Lytkina, N.I. Shulakova, V.V. Romanenko, A.I. Yurovskikh, A.A. Yasinsky //Hepatology. – – No. 1. – P.34-40.
- Carey D. The prevalence and natural history of hepatitis B in the 21st century / Cleve. Clin Med., 2009. - N 76 (Suppl. 3). – P. 2 – 5.
- Dienstag JL Drug Therapy: Hepatitis B Virus //N. English J. Med., 2008. - Vol 359, N. 14. - R. 1486-1500.
- European Association for the Study of the Liver (EASL), Clinical Practice Guidelines: Management of chronic hepatitis B. //J. Hepatol., 2009.– No. 50(2). - R. 227-242.
- Elgouhari M., Abu-Rajab Tamimi TI, Carey WD Hepatitis B virus infection: understanding its epidemiology, course, and diagnosis/ Cleve. Clin. J. Med., 2008. - N 75 (12). - P. 881 - 889.
- Lok S., McMahon BJ Chronic hepatitis B: update 2009 / Hepatology, 2009. – N 50 (3). – P. 661-662.
- Mitchell AE, Colvin HM, Beasley RP Institute of Medicine Recommendations for the Prevention and Control of Hepatitis B and C / Hepatology, – Vol.51 (N 3). - P. 729-733.
UDC: 616.36-002-022.7-07:578.27:578.891
APPLICATION ENTEROSORBENT “ATOXYL” IN THE TREATMENT OF PATIENTS ON SEVERE HEPATITIS AND AND IN
IN articles is being held analysis own effectiveness studies therapies 37 sick on hepatitis AND and IN enterosorbent Atoxyl, who were treated in the clinic of infectious diseases of the National Medical University in 2011 - 2012. The results of treatment were compared with the corresponding indicators in 36 patients of the comparison group, which had the same composition in terms of age, gender, severity of the course, and the nature of the concomitant pathology. The results obtained indicate the feasibility of treating patients with GA and acute GV with a non-severe course of the disease with Atoxyl, which allows to significantly reduce the duration of the intoxication period, jaundice, and reduce the level of total and direct bilirubin in the blood compared to the corresponding indicators in patients who did not receive enterosorbents. The drug was well tolerated by patients and did not cause serious side effects.
O.A. Golubovska, M.Ch. Korchinsky
UDC: 616.36-002-022.7-07:578.27:578.891
ENTEROSORBENT "ATOKSYL" USE IN THE TREATMENT OF PATIENTS WITH ACUTE HEPATITIS A AND B
In the article the analysis of their research the effectiveness of therapy 37 patients with hepatitis A and B enterosorbent Atoksyl who were treated at the clinic of infectious diseases NMU in 2011 - 2012. Results of treatment compared with the cor-responding parameters in 36 patients with comparison group who had the same composition by age, sex, severity, nature of comorbidity. The results demonstrate the feasibility of a treatment Atoksyl patients with hepatitis A and acute hepatitis B with no serious disease, which allows to significantly reduce the intoxication period, jaundice, reduced levels of total and direct bilirubin levels compared with the corresponding rates in patients not receiving enterosorbents. The drug was well tolerated by patients and did not cause serious side effects.
Golubovskaya, M. Korchynskyi